Diagnosing and Treating Tachycardias
Premature Complex
The early depolarization of myocytes causes premature complexes. Many patients may sense these as palpitations. If these are frequent, it may be a harbinger of either a supraventricular or ventricular tachycardia. While individual premature complexes are generally benign, they may signal an underlying heart condition or external factors that need treatment.
Premature Atrial Complexes (or PACs)
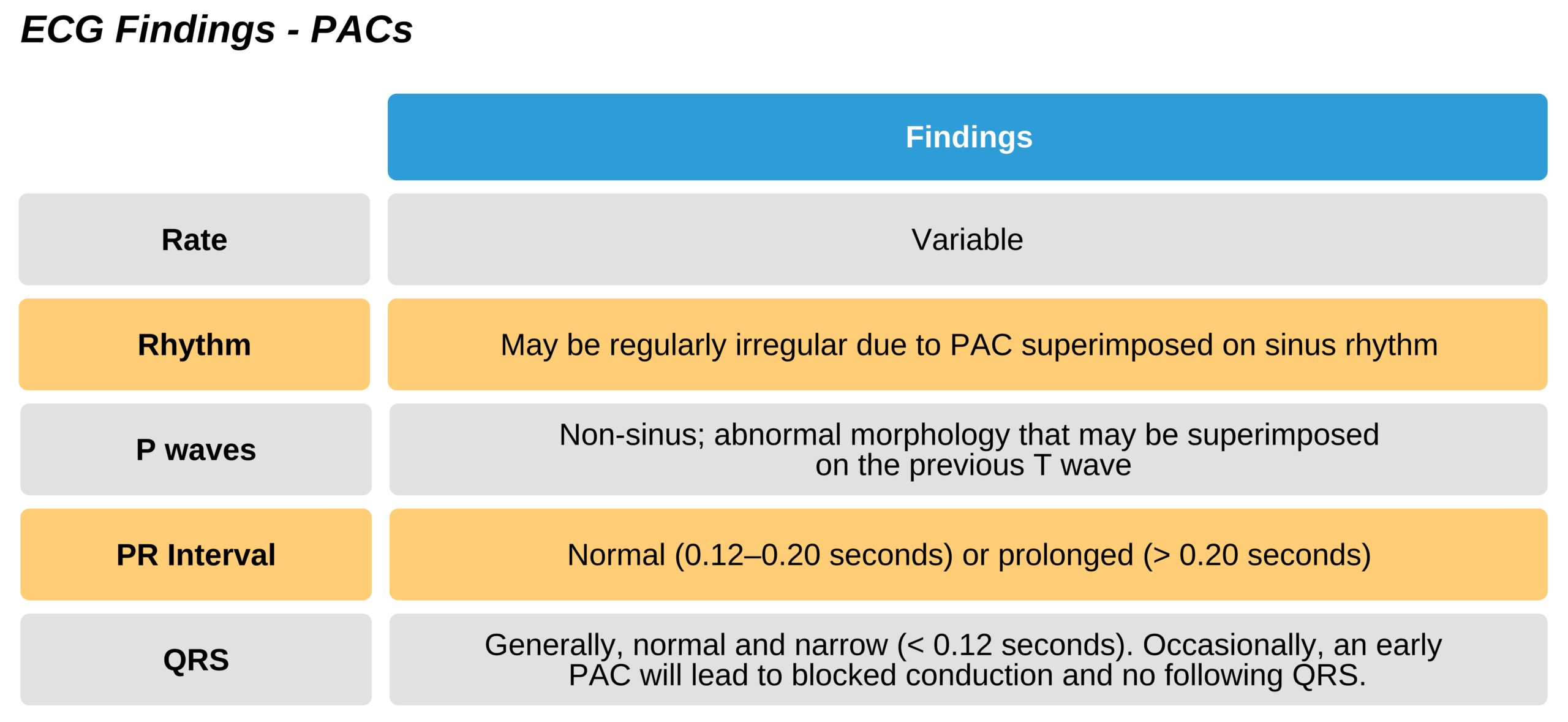
PACS are quite common and are noted on ECG as an early P wave with either a normal or long PR interval (if they are very premature). A PAC may look a bit different than a normal sinus wave, but this may not be easily distinguishable. The PAC can disrupt the normal sinus rhythm, causing a pattern irregularity or a regularly irregular pattern.
When a QRS complex does not have a preceding P wave, the previous T wave can be checked to see if it looks abnormal; there may be a premature superimposed P wave. This happens when a premature P wave occurs at the relative refractory or complete refractory time so that the conduction is blocked or slowed. Either no QRS will follow, or the PR interval will be long. This is commonly seen when the RP interval (time between QRS to subsequent P wave) is short, and it can be mistaken for heart block
Related Video: ECG Rhythm Review: Premature Atrial Complex (PAC)
Pathophysiology
PACs are due to non-sinus node atrial depolarizations. Consequently, they can instigate a paroxysmal SVT. Generally, PACs are benign and only felt as palpations. Occasionally, the PAC may depolarize the SA node, leading to a delay before the next sinus P wave.
Symptoms and Signs of PACs
- Generally asymptomatic
- Occasionally sensations of palpitation or skipped heartbeat
Underlying Causes
Commonly, PACs are due to medications and stimulants, including caffeine, methamphetamines, and drugs containing ephedrine. Noncardiac disease states may also cause PACs, such as hypovolemia, hyperthyroidism, or fever.
Management
- Typically, no treatment is needed except the management of the underlying condition or abstaining from drugs.
Related Video: One Quick Question: What are PACs (Premature Atrial Contractions)?
Premature Ventricular Complexes (or PVCs)
Pathophysiology
PVCs are caused by depolarizations within the ventricle that precede the impulse conducted by the SA node. This may be due to a focus of automaticity, an unstable impulse, or a reentry circuit.
Related Video: ECG Rhythm Review – PVCs
Premature Ventricular Contractions (PVC)
Related Video: One Quick Question: What are PVCs (Premature Ventricular Contractions)?
Anatomy of PVCs
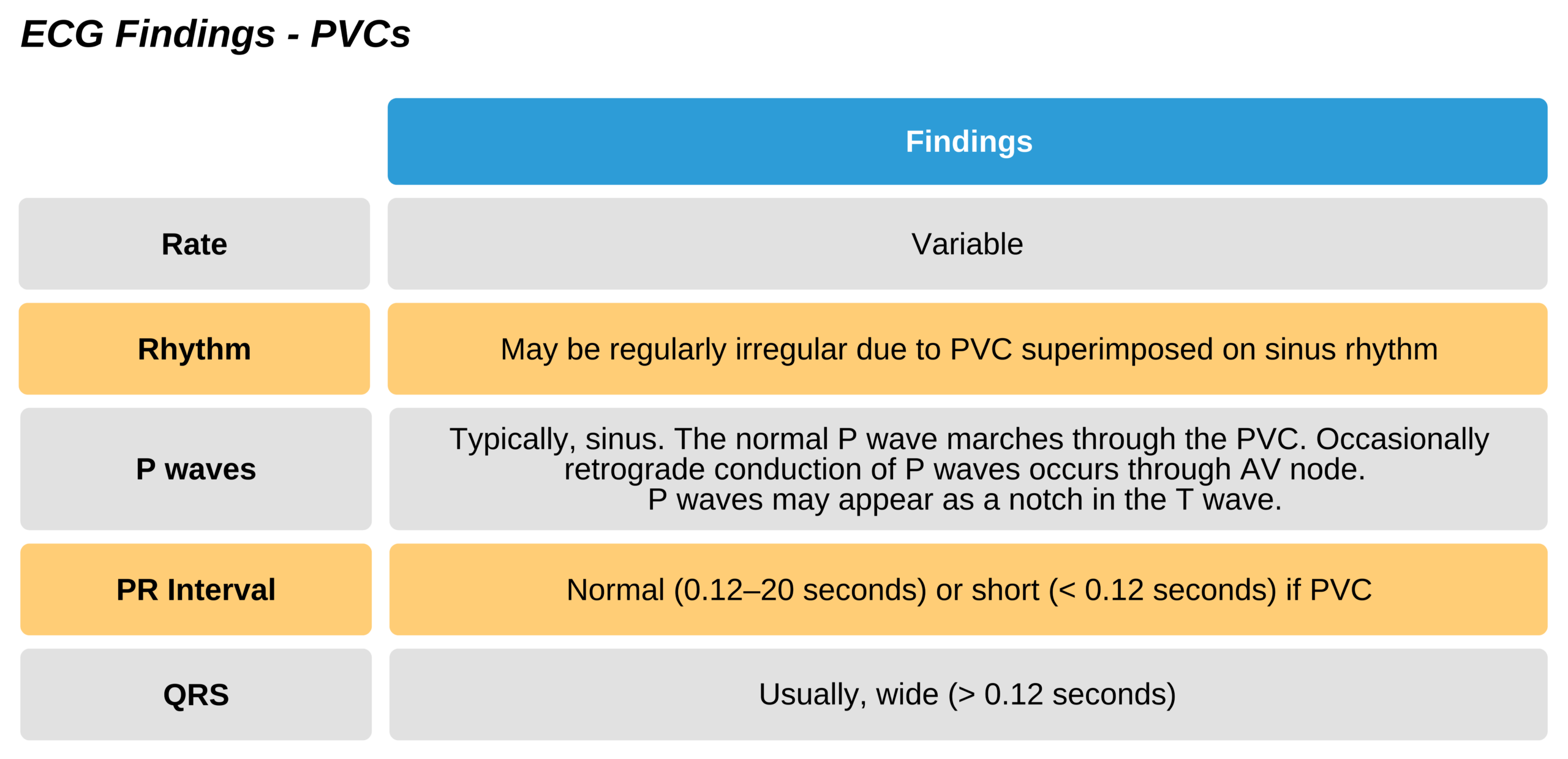
Abnormal and wide: PVCs change the normal QRS morphology as they do not use the standard pathway through the AV node and Purkinje fibers. Instead, PVCs take a slower pathway that leads to wide (> 0.12 sec) and abnormal appearing QRS complexes. Additionally, repolarization is abnormal, leading to ST segment and T wave changes.
Relationship to P wave: PVCs are initiated below the sinus node and are independent of the SA node. Therefore, usually there is a sinus P wave that is unaffected by the PVCs (unless the PVC can pass retrograde through the AV node back to the atria). Consequently, normal P waves will frequently be seen marching through the abnormal ventricular beats in a normal sinus rhythm.
There are also additional specific characteristics of the PVC, including a compensatory pause and the QRS morphology, but these characteristics are not universal. Of note, sometimes supraventricular rhythms can appear wide and be mistaken for PVCs. A PVC rarely may be initiated in the Purkinje fibers and have a narrow QRS.
Compensatory Pauses: PVCs may occur during a specific time interval that blocks the conduction of the following P wave so that no QRS is generated. Thus, there will be a pause (no QRS) between the two following P waves. As this only happens during a certain time interval, this compensatory pause does not always occur with PVCs and is not a meaningful finding for diagnosis.
Bi- and Trigeminy: if PVCs originate in the same ventricular location, their morphology may be the same. These are termed unifocal. If the second QRS is always a PVC, it is termed ventricular bigeminy. If the third QRS is always a PVC, it is known as ventricular trigeminy. Ventricular quadrigeminy occurs when every fourth QRS is a PVC and on and on.

Bigeminy Premature Ventricular Complex ECG

Trigeminy Premature Ventricular Complex ECG
Related Video: One Quick Question: How Can I Remember the PVCs?
Period of Vulnerability and R-on-T Phenomena: T waves coincide with the repolarization of the ventricle. During this time, there is a period that is absolutely refractory followed by a period that is relatively refractory to another depolarization. In the former, no depolarizations can occur. However, in the latter, the cells are somewhat unstable considered to be in a period of vulnerability.
Traditionally, a PVC during the vulnerable period was thought to lead to unstable ventricular tachycardias such as VF or VT. However, research now suggests that PVCs occurring at any time during the cardiac cycle can lead to these arrhythmias. Instead, certain factors may lead to VF or VT, such as a long QT interval due to electrolyte imbalances or drug overdoses.
In patients with a predisposing condition, a prolonged R interval (due to bradycardia) can incite a PVC, which then superimposes on the T wave (R-on-T phenomena). This may then initiate polymorphic VT (e.g., torsades de pointes).

PVC With Prolonged RR Interval Leading to V-Tach or VF
Premature Junctional Complexes (PJCs)
Pathophysiology
PJCs are electrical impulses incited at the AV node before the subsequent sinus conduction. These are a relatively less common type of premature beat. Due to their location at the AV node, the impulse may be anterograde or retrograde. In the case of retrograde conduction, the P wave can follow, be embedded in, or come before the sinus QRS. This depends on the location within the AV node as well as the relative speed of retrograde versus anterograde conduction. The P waves from the PJC will be abnormal compared to sinus P waves. A retrograde P wave will alter the PR interval length. Typically, the QRS is narrow unless there is a coinciding conduction pathway abnormality (e.g., bundle branch block).
Related Video: One Quick Question: What are PJCs (Premature Junctional Contractions)?
Related Video: One Quick Question: What are the Junctional Escape Rhythm Criteria?

Premature Junction Complex ECG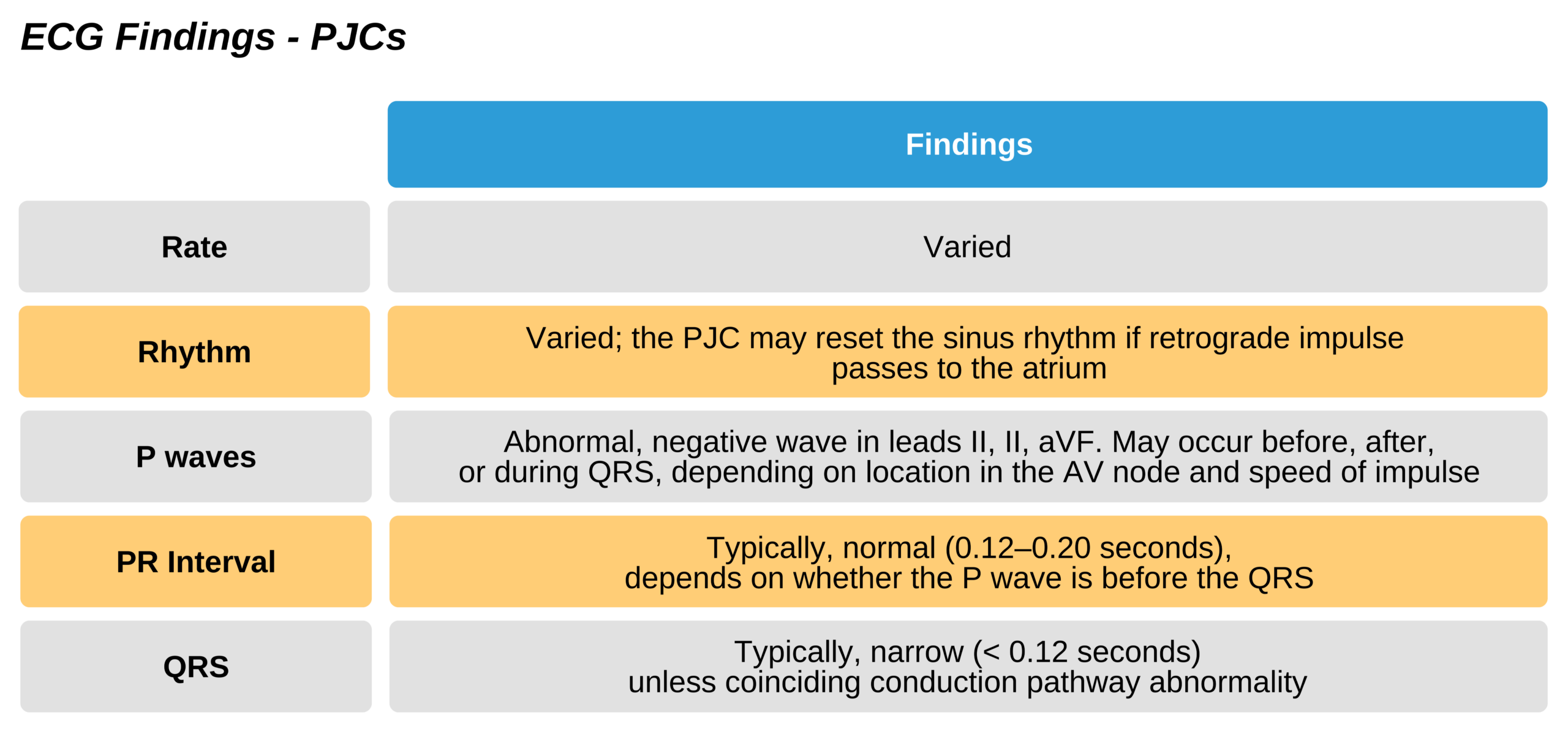
Narrow Complex SVTs
These arrhythmias can arise from a range of conditions. Typically, the underlying diagnosis should be defined if the patient is stable to determine the best treatment plan.
There are usually four major categories for narrow complex SVTs.
- Sinus tachycardia
- Atrial fibrillation and flutter
- Reentry SVT
- Automated atrial arrhythmia (not reentry). Examples include ectopic and multifocal atrial tachycardias.
Usually, a quick diagnosis can be made. If not, a more thorough evaluation of the ECG can help to verify the diagnosis.

Supraventricular Tachycardia ECG
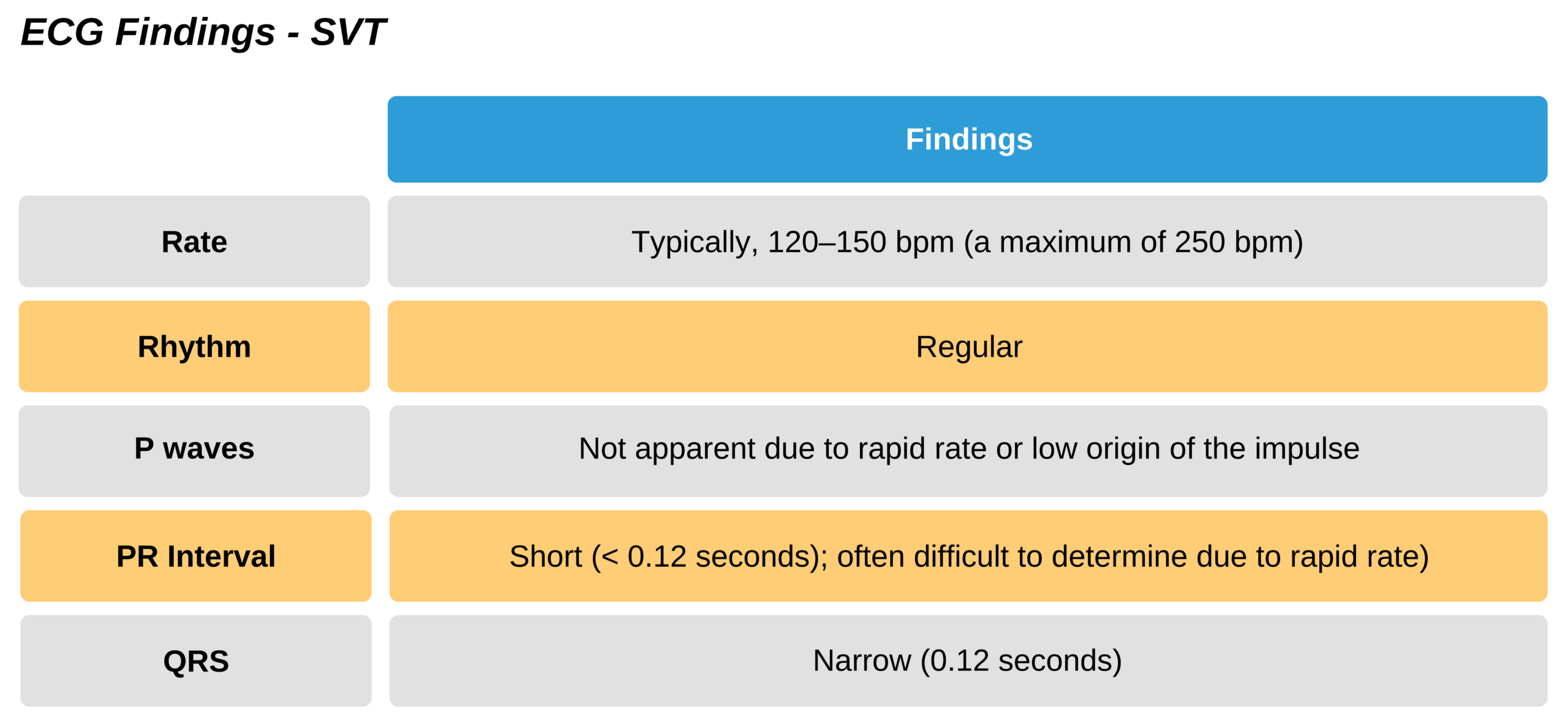
ECG Findings
The diagnosis is determined by evaluating the characteristic features. Typically, three areas of the ECG are reviewed:
- Rate regularity
- P waves
- PR interval
Characterizing a narrow complex SVT with a regular rate:
- Normal P wave and PR interval: usually sinus tachycardia or ectopic atrial tachycardias
- Flutter waves (and stable AV block): atrial flutter
- No P waves and short PR interval: reentry SVT and (less often) junctional tachycardia
Assessing a narrow complex SVT with an irregular rate:
- Irregularly irregular: atrial fibrillation
- Flutter waves (and variable AV block): atrial flutter
- Multifocal atrial tachycardia
Related Video: One Quick Question: What are the SVT (Supraventricular Tachycardia) Criteria?
Related Video: One Quick Question: What are the Differences Between ST (Sinus Tachycardia) and SVT?
Evaluating Adenosine and Vagal Stimulation
Additionally, using diagnostic (and therapeutic) maneuvers such as IV adenosine or vagal stimulation can help determine the type of regular and narrow complex SVT. The response to each arrhythmia is different:
- Paroxysmal SVT: the sudden resolution of tachycardia as the reentry circuit conduction is blocked
- Atrial tachycardia/atrial flutter: temporary AV block and slowed ventricular rate with the persistence of atrial arrhythmia or abnormal P waves
- Sinus tachycardia: temporarily slowed rate and AV block
- Junctional tachycardia: temporarily slowed rate
Note that irregular narrow complex SVTs are typically easy to identify on ECG and do not usually require these maneuvers for diagnosis.
Wide Complex SVTs
- When a supraventricular tachycardia has a wide complex, it is managed as a narrow complex SVT. This is usually with aberrancy.
- A wide complex ventricular tachycardia is managed along with the algorithm for tachycardia with a pulse. A cardiology consultation should be obtained.
- A wide complex of unknown origin will require cardiology consultation. Managing these arrhythmias without understanding the origin can lead to worsening of the arrhythmia if the incorrect antiarrhythmic agent is used.
Sinus Tachycardia
Pathophysiology
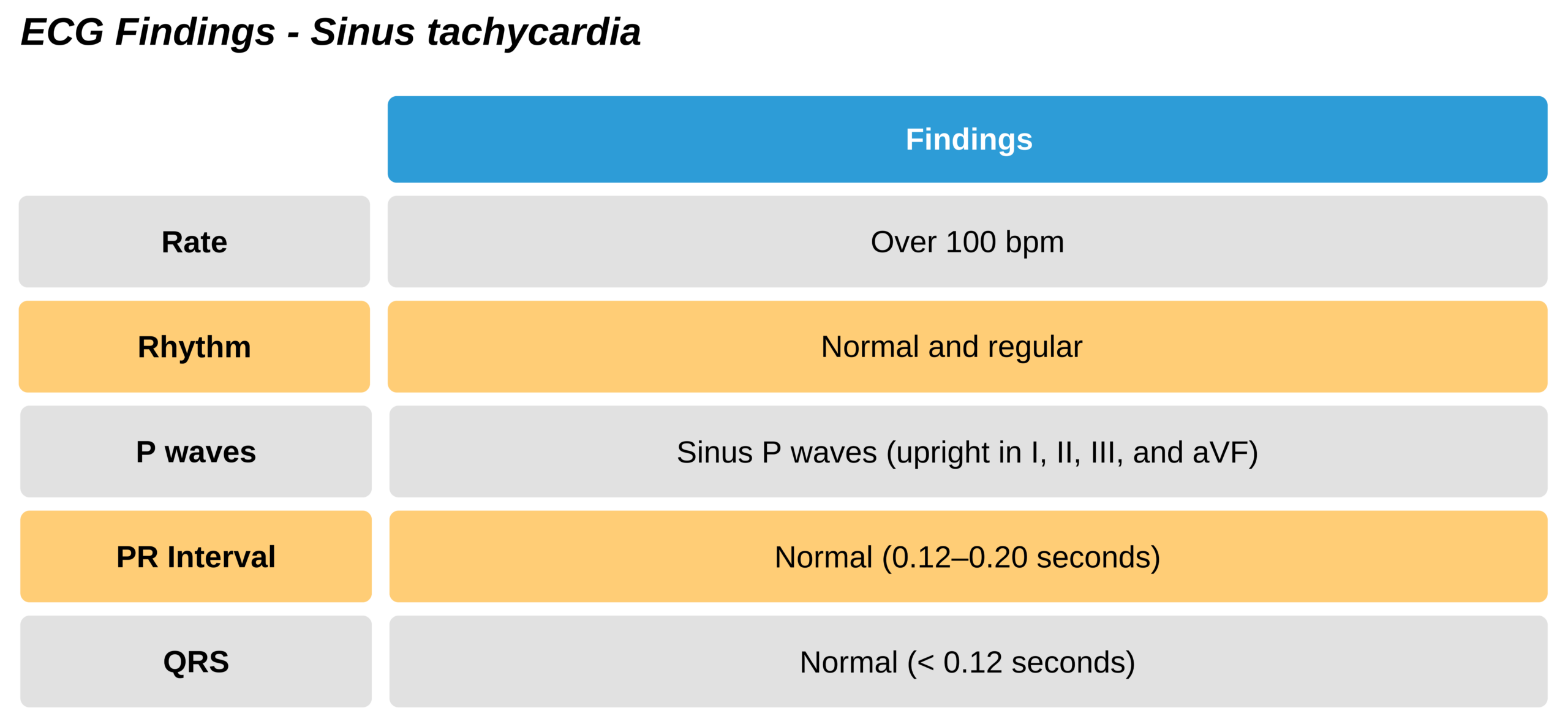
Typically, sinus tachycardia is a physiologic response to a condition or situation and is usually an appropriate response. Very rarely, there may be no underlying cause or situation associated with the tachycardia, and then it would be considered an arrhythmia. Typically, the normal upper limit of heart rate is calculated by subtracting the patient’s age in years from 220 bpm.

Sinus Tachycardia With Regular Rate and Rhythm ECG
Related Video: ECG Rhythm Review – Sinus Tachycardia
Symptoms and Signs of Tachycardia
Patients may experience palpitations. Additionally, there may be symptoms and signs of the underlying condition predisposing the patient to tachycardia.
Underlying causes
Common causes include:
- Exercise
- Fever
- Hyperthyroidism
- Adrenergic overactivity
- Anemia
- Hypovolemia
Management
There is no standard treatment for sinus tachycardia. It is usually managed by treating the underlying cause. A fast heart rate alone should not be treated, as in a physiologic response. The elevated heart rate may be helping to maintain cardiac output if the stroke volume is suboptimal.
- Of note, if sinus tachycardia has no underlying cause, treatment may include medications that slow the heart rate, such as beta-blockers, calcium channel blockers, and radiofrequency ablation.
- Cardioversion or defibrillation should not be attempted in sinus tachycardia. These treatments are useful for producing sinus rhythms and will not improve a rhythm that is already sinus.
Reentry SVT
These narrow complex SVTs have a wide range of morphologies and mechanisms of actions due to their various sites of origin. A subtype, known as paroxysmal SVT, begins suddenly, lasts longer than a few beats, and then suddenly ends.
These reentry arrhythmias may be conducted via the AV node, termed AV node reentry tachycardias (AVNRT). Alternatively, they may be conducted via the AV node along with an alternative pathway, also known as AV reentry tachycardias (AVRTs). AVNRTs are the most common form of reentry tachycardias in adults and usually allow both anterograde and retrograde conduction.
Pathophysiology
Reentry SVTs occur due to multiple conduction pathways. When this occurs at a specific time in the pathway, the impulse can cycle in a continuous circuit. When this occurs within the AV node only, it becomes an AVNRT.
Related Video: ECG Rhythm Review – Supraventricular Tachycardia (SVT)

Reentry Pathway
Symptoms and Signs
- Palpitations leading to anxiety and discomfort
- Exercise intolerance
- Shock and instability
Underlying causes
- Alternate conduction pathway
- Stimulants and environmental factors including caffeine, cigarettes, hypoxia, anxiety, loss of sleep, and polypharmacy
- It is also increased in patients with cardiac and pulmonary disease (CAD, obstructive pulmonary disease, heart failure)
Management
Initially, if the underlying diagnosis is not known, a trial of adenosine or vagal maneuvers, followed by:
- In a healthy patient with normal cardiac function:
- Blocking the AV node with
- beta-blockers
- calcium channel blockers
- digoxin
- Cardioversion
- IV antiarrhythmic, including
- procainamide
- amiodarone
- sotalol
- Blocking the AV node with
- In patients with heart failure:
- Cardioversion
- Digoxin
- Amiodarone
Reentry occurs due to these underlying conditions:
- When two or more conductive pathways exist between the origin site and an end destination. When within the AV node, one will be fast and the other slow.
- The conductive pathways have different properties, including different refractory periods and conduction.
- The electrical impulse, which is usually early, approaches the two pathways, allowing reentry:
- The conductive pathway still in its refractory period is unable to allow anterograde conduction.
- The slower conductive pathway allows anterograde conduction at a speed coinciding with the end of the first pathway’s refractory period.
- This very specific timing allows the impulse to continuously circle along these two pathways in a circuit that never encounters a refractory period. Each time around the pathway stimulates an impulse that, with enough repetition, can eventually become a tachyarrhythmia. Within the AV node, this will lead to AVRNT.
Underlying Mechanism of Tachycardias
Narrow Complex SVTs usually arise one of two ways:
Automaticity: in these, there is simply increased impulse generation. These include sinus, junctional, ectopic atrial, and multifocal atrial tachycardias. Cardioversion is not effective for these arrhythmias.
Reentry: in these, a reentry circuit exists. These include atrial fibrillation and flutter, as well as paroxysmal SVT. Cardioversion is used for these arrhythmias. Reentry usually occurs in these three areas:
- Atrium: atrial fibrillation and flutter
- AV node: AVNRT
- AV node and an alternative conductive pathway: AVRT.

Different ECG Reentry Pathways
Paroxysmal SVT
These sudden start-stop reentry SVTs occur due to AVNRT and AVRT and usually occur at rates > 150 bpm. P waves are often difficult to identify. Additionally, the AV node typically provides anterograde conduction while the alternate pathway allows retrograde conduction. This is referred to as an orthodromic and reciprocating tachycardia. If the opposite is true, AV node conducts retrograde and alternate pathway conducts anterograde, the QRS will appear wide. This is known as antidromic reciprocating tachycardia.
Management
Initial therapy for paroxysmal SVT is a vagal maneuver. Adenosine is also useful for blocking AV node conduction both anterograde and retrograde and stopping the reentry circuit.
Valsalva
This maneuver has been used since the 1600s. It involves forcefully exhaling while obstructing the glottis so there is no air escape.

Valsalva Maneuver
Valsalva causes a sudden increased pressure within the abdomen and thorax. Typically, asking the patient to bear down while closing the mouth and nostrils will suffice. During the maneuver:
- Arterial pressure rises.
- Increased pressure triggers local baroreceptors.
- Baroreceptors send a signal to the brain, which then increases parasympathetic tone.
- Vagal tone increases, resulting in decreased heart rate and conduction via the AV node.
- This can stop reentry tachycardias or cause a temporary AV nodal block.
Success with vagal maneuvers ranges between 6% and 18 % when used outside of the hospital. These rates may be higher in specialized laboratory settings. Other conditions may worsen their success rate:
- Patient’s lack of understanding or inability to perform the maneuver
- Comorbid cardiac dysfunction or increased adrenergic stimulation
Valsalva can also be used in combination with massage of the carotid sinus. While equally effective, one may work where the other failed.
To perform the Valsalva maneuver:
- The patient may stand up or remain seated. Cardiac monitoring and IV access should be initiated in case of a significant bradycardic response.
- The clinician instructs the patient on the maneuver and to cough at will, as this can blunt the effect of vagal maneuvers if needed.
- Initial vitals are assessed, including heart rate, blood pressure, and cardiac rhythm.
- The patient is instructed to inhale deeply then hold the breath while bearing down. The patient can also blow into a tube or a syringe attached to a manometer or use spirometry. (Goal pressure should be 30 mm Hg.) As an alternative, the clinician can press firmly on the abdomen (without causing pain) and have the patient push against the resistance.
- The patient should strain for 15–30 seconds while holding their breath.
- Subsequent heart rate and blood pressure are recorded at 1 minute. The cardiac rhythm is then reevaluated with a rhythm strip. Resolution should be confirmed with a 12-lead ECG.
- If unsuccessful, carotid sinus massage can be attempted.
Massage of Carotid Sinus (CSM)
The carotid sinus is an area of the common carotid artery that lies at the junction of the external and internal carotid arteries. Within it are baroceptors that measure carotid artery pressure changes. It contains endings of the glossopharyngeal nerve (cranial nerve IX) that communicate with the area of brainstem that controls the heart and other vasomotor activity. The outflow is to the vagus nerve, which causes increased parasympathetic activity, leading to slowed activity of the SA node and slowed conduction of the AV node. The result is a slowed heart rate and may cause a temporary AV node block.
This mechanism is called a vasovagal response because the carotid (or vasal component) activates the brain and then mediates the vagus nerve (or vagal component) to slow the heart. This can additionally lead to dilation of the peripheral vasculature. Consequently, this maneuver can cause hypotension by both a slowed heart rate and vasodilation.

Carotid Sinus Massage
When preparing for carotid sinus massage:
- The procedure should be limited to young, healthy patients with no history of vascular disease that could put them at risk for dislodging a plaque within the carotid artery during the procedure.
- Cardiac monitoring and IV access should be in place in the case of significant bradycardic response. Atropine and transcutaneous pacers should also be available in case of significant bradycardia.
- The clinician ensures there is no history of vascular disease (including stroke, recent MI, ventricular arrhythmias). There should be caution when considering this procedure in older individuals due to the greater likelihood of vascular disease. The patient has no recent carotid surgery or a carotid bruit.
Key Takeaway
Choose massage of the right carotid sinus in a right-handed patient. If the person is left-handed, choose the left carotid sinus.
When performing CSM:
- The maneuver is performed on the right carotid by turning the head to the left. In the case of a carotid embolic event, a right-sided embolus would affect the non-dominant side of the brain in the majority of right-handed patients.
- Cardiac monitoring is initiated and vital signs recorded.
- The carotid sinus is palpated at the level of the carotid pulse between the angle of the jaw and sternocleidomastoids.
- The clinician uses two fingers to press firmly on the carotid sinus and massages vertically with the pressure directed posteromedially for 5–10 seconds.
- This is repeated 2–3 times with 5–10 second interruptions.
- A cardiac rhythm strip should be recorded before and after to check for a response. This is confirmed with a 12-lead ECG.
- If unsuccessful, the procedure can be done on the left side, if the patient’s vitals are stable.
- Massage can be attempted a few times before determining its effectiveness.
- The clinician should never massage both sides as this can severely diminish the brain’s blood flow.
- The procedure may be combined with Valsalva if unsuccessful.
This maneuver can have complications, but they are rare at < 0.5% in acceptable candidates with good technique. Some complications are:
- Embolic event (TIA and stroke)
- Syncope
- Asystole
- Sinus arrest
- AV block or paradoxical tachyarrhythmias in patients with digoxin toxicity
Most complications are temporary and resolve within 24 hours. Regardless, the clinician should be prepared and have IV access before performing this maneuver.
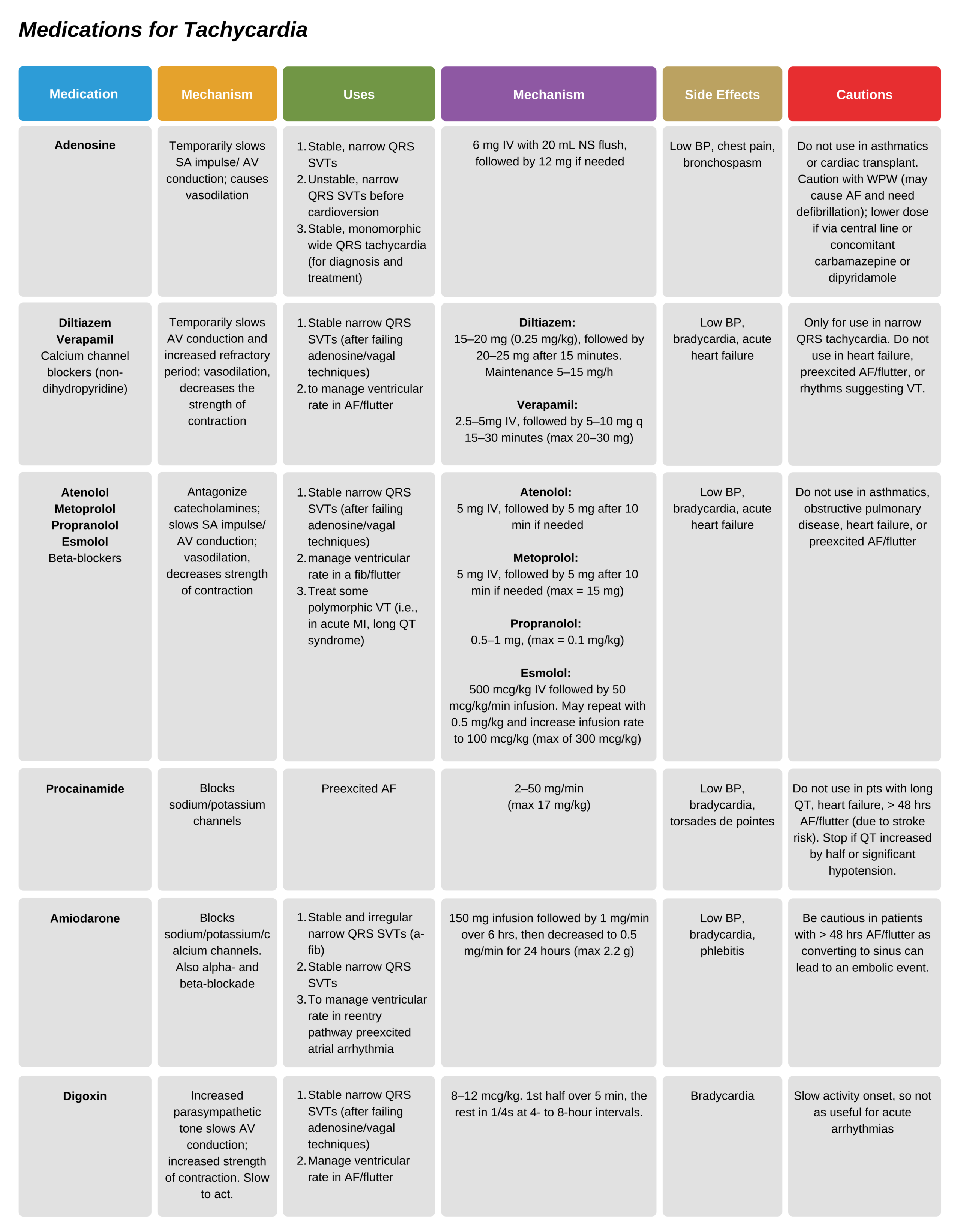
Adenosine
Adenosine can be used to manage reentry SVTs that are unresponsive to vagal techniques. The dosage is 6 mg IV/IO via large veins over 1–3 seconds, followed by a saline flush. A follow-up dose of 12 mg can be given after 1–2 minutes if not responsive. While higher dose adenosine can be used, if these two doses are ineffective, consultation with cardiology is prudent.
Adenosine is not used for tachyarrhythmias that are irregularly irregular, especially in those with a wide QRS. These may be ventricular arrhythmias, and adenosine can precipitate atrial fibrillation in patients with WPW preexcitation. Defibrillators should be available in case of this scenario.
Mechanism of action: adenosine is essentially the medication equivalent to vagal techniques. Adenosine stimulates its specific receptors, which reduce impulse generation and conduction in the SA and AV nodes. The effect can be the termination of paroxysmal SVT, and studies show that at 6 mg doses (with 12 mg follow-up as needed), 57–93% of cases are successfully treated.
Diagnosis of SVTs: Adenosine can help diagnose cases of SVT. This is useful in atrial fibrillation or flutter as slowing of AV node conduction can help reveal the atrial arrhythmia. While this is not usually needed for diagnosis of irregularly irregular ventricular arrhythmias, atrial flutter can masquerade as regular rhythm SVT. When administering adenosine, it is vital to have IV access and cardiac monitoring.
Side Effects: There are complications associated with adenosine. It can interact with other medications, and the dose may need to be increased in patients on adenosine antagonists (e.g., caffeine, theophylline) and decreased in patients with adenosine agonists (e.g., carbamazepine, dipyridamole) or when given through a central vein. Additionally, patients on certain heart medications such as beta-blockers, diltiazem, and verapamil may need a lower dose as these cause an additive bradycardic effect.
Side effects are frequently seen and include flushing, chest pain, and shortness of breath. Susceptible patients may have a significant bradycardic response and need transcutaneous pacing. Adenosine may be contraindicated in patients with asthma, who are at risk of bronchospasm, as well as patients with cardiac transplant as they may have significant sensitivity to adenosine, leading to asystole. Typically, adenosine is safe to use during pregnancy.
Beta-Blockers and Calcium Channel Blockers
Following the failure of vagal techniques and adenosine, the next step in management would be the use of long-acting medications that block the AV node. These include the non-dihydropyridine class of calcium channel blocker (diltiazem and verapamil) and beta-blockers.
Related Video: Verapamil vs Cardizem – ACLS Drugs
Mechanism of action: Both medication types work by blocking reentry circuits that use the AV node or by decreasing AV node conduction and the ventricles’ response to SVT. These medicines work longer than adenosine and thus have sustained effects. Studies show that they are effective in treating paroxysmal SVTs.
Beta-blocker medications (including atenolol, metoprolol, propranolol, esmolol) oppose the sympathetic effect on the SA and AV nodes, resulting in a decreased rate of conduction. They reduce the contraction force of the heart and lead to worsened cardiac output in heart failure.
Side Effects: the calcium channel blockers should only be given in narrow QRS tachycardias that are known to be supraventricular. Patients with wide QRS tachyarrhythmias, reduced cardiac output, and heart failure should not be given verapamil.
Beta-blockers should not be used in patients with obstructive pulmonary disease or heart failure. These medicines can lead to hypotension, delay in AV node conduction, and bradycardia.
- Caution is recommended when managing patients with pre-excited atrial arrhythmias conducting through an alternative pathway and the AV node. A medication that blocks the AV node will likely not manage the ventricular rate and may increase it. Cardiology should be consulted in these cases.
- Caution is recommended when using multiple long-acting AV node blocking agents. These can lead to severe bradycardia.
Related Video: Adenosine – ACLS Drugs
Related Video: Amiodarone – ACLS Drugs
Related Video: Lidocaine – ACLS Drugs
Managing Atrial Fibrillation (AF)
When managing atrial fibrillation and flutter, clinicians should follow these steps (in order of importance):
- Emergent synchronized cardioversion in unstable patients
- Ventricular rate control
- Anticoagulation before and following cardioversion in patients with AF or flutter > 48 hours duration. This decreases the chance of emboli.
Pathophysiology
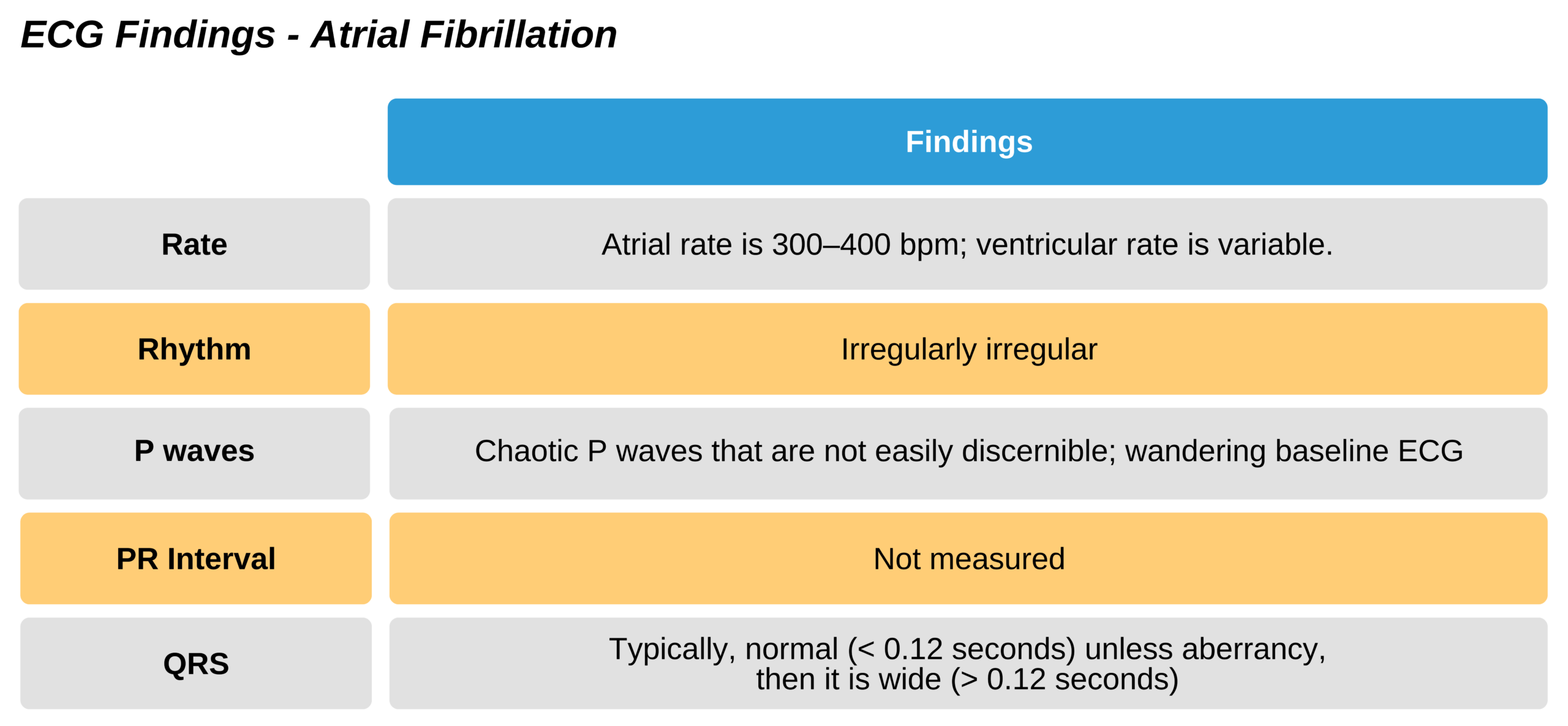
Atrial fibrillation arises from impulses that are more rapid than the SA node and occurs via reentry circuits. Atrial fibrillation is the most common persistent arrhythmia. In atrial fibrillation, the atrial impulse takes many random and chaotic pathways, which lead to irregularly irregular and very rapid ventricular depolarizations. Consequently, the atrial rate can be up to 400 beats per minute, which is too fast to allow for effective atrial contractions. At this rate, no true P waves are seen.
There is a baseline change in the ECG due to the abnormal electrical impulses, and this leads to a fibrillation pattern. Due to the chaotic nature of the electrical impulses, not all are effectively conducted, leading to an irregular rhythm. Since not all impulses are conducted, this limits the ventricular rate.

Atrial fibrillation is an irregular and often rapid heart rate.
Related Video: ECG Rhythm Review – Atrial Fibrillation

Atrial Fibrillation ECG With Irregular, Wandering Baseline
Symptoms and Signs
- Typically, patients will have a feeling of palpitations due to the irregular rhythm. They may also have dizziness, fatigue, weakness, and dyspnea with exertion.
- Patients may be asymptomatic.
- AF can cause thrombi due to the stasis of the atrial blood. As a result, patients may initially present with a thromboembolic event with signs and symptoms of a stroke.
- Symptoms can depend on the ventricular rate, cardiac output, and function.
- If there is rapid ventricular response (i.e., many atrial impulses cause ventricular contractions), patients may have more symptoms of tachycardia, including hypotension, dyspnea, chest pain, and pulmonary edema. This usually occurs with ventricular rates > 150 bpm.
- Due to the lack of atrial contraction (and instead, ineffective fibrillation), there can be a significant decrease in cardiac output with low cardiac perfusion. Atrial contractions contribute about ¼ of the filling of the ventricles and, in a vulnerable person, can lead to a symptomatic decrease in cardiac output.
- Coexisting WPW syndrome: in patients that have a preexcitation syndrome, such as WPW, atrial fibrillation (and flutter) can cause very rapid conductions due to the existing alternate conduction pathway. These patients have very rapid and irregular wide-QRS tachycardias that may resemble VT. A history of WPW or a variation in the QRS complex can help provide a clue to this diagnosis.
Underlying Causes
AF is usually related to some form of cardiac disease. However, it can occasionally occur in a normal heart.
Common causes include:
- Coronary disease, ACS, and heart failure
- Valvular cardiac disease (mitral, tricuspid valves)
- Medication-associated (digoxin, quinidine)
- Hyperthyroidism
- Pulmonary emboli
- Sick sinus syndrome
- Pericarditis
There are certain reversible conditions associated with atrial fibrillation that can be treated:
- Hypoxia
- Hypertension
- Mitral valve insufficiency
- Shock, hypovolemia
- Anemia
- CHF
- Thyrotoxicosis
- Electrolyte abnormalities (potassium, magnesium)
- Drugs (stimulants, alcohol)
Key Takeaway
Underlying causes for AF –
it is usually associated with an underlying cardiac condition.
Look for comorbid conditions or triggers that are reversible.
Management
The ACLS responder does not treat stable atrial fibrillation. Instead, these patients should be managed by cardiologists to determine the best long-term therapy.
However, sudden onset or unstable atrial fibrillation must be managed acutely. Important questions to ask include:
- Is the patient stable?
- Unstable patients should be treated urgently.
- Is there a normal cardiac function?
- The heart rate needs to be slowed if there is poor cardiac function.
- Is WPW present?
- The patient should undergo cardioversion to convert to a normal rhythm.
- Has the duration been more than 48 hours?
- The patient should be anticoagulated.
Unstable patients are managed with cardioversion. Patients who are more stable can be managed using rate control with beta-blockers and nondihydropyridine calcium channel blockers. Patients with WPW syndrome should not be given AV nodal blocking agents.
To control the ventricular rate:
- Patients with normal cardiac function are treated with:
- calcium channel blockers (diltiazem or verapamil) or beta-blockers (e.g., metoprolol)
- Patients with abnormal cardiac function (e.g., heart failure) are treated with:
- amiodarone or digoxin
To convert the rhythm:
- If under 48 hours – cardioversion, amiodarone
- If over 48 hours – anticoagulation for 3 weeks, then cardioversion. Anticoagulation is then continued for another 4 weeks.
- In patients with normal cardiac function, an alternative is IV heparin, given after a transesophageal echocardiogram to rule out an existing clot. The patient is then cardioverted within the next 24 hours and anticoagulation continued for another 4 weeks.
Cardioverting a patient who has been in atrial fibrillation or flutter for more than 48 hours increases the risk of moving a preexisting clot. This should only be considered in an unstable patient or after consulting cardiology (i.e., with transesophageal echo to evaluate for a clot)
Key Takeaway
Caution with Adenosine
Do not give adenosine in patients who are unstable or have polymorphic wide QRS tachycardia as this can precipitate VF.
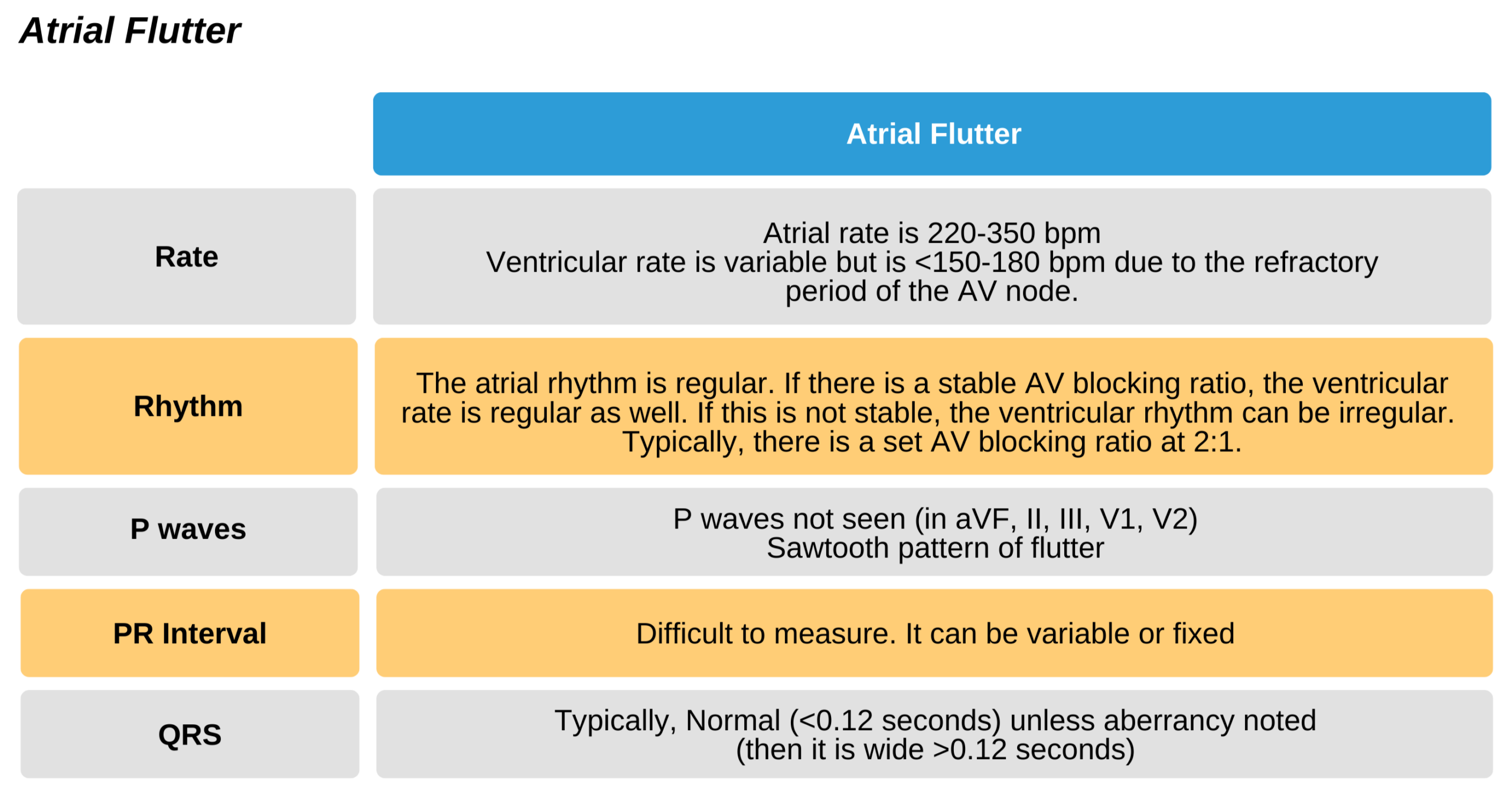
Managing Atrial Flutter
Like atrial fibrillation, atrial flutter arises from impulses that are more rapid than the SA node and circulates via reentry circuits.
In contrast, in atrial flutter, the reentry circuit is a single circuit within the atrium that leads to a flutter pattern. This is often called a sawtooth pattern and can be seen well in leads aVF, II, and III.
-
Symptoms and Signs
- As in atrial fibrillation
Underlying causes
Typically, atrial flutter is associated with underlying cardiac disease. Common cardiac diseases include valvular cardiac disease, coronary disease, and cor pulmonale. It is rarely seen in a structurally normal heart.
Management
Atrial flutter is usually managed similarly to atrial fibrillation.
Adenosine is too short-acting to manage atrial flutter (or fibrillation). Still, it can be used for diagnosis, although this is rarely needed.
Related Video: ECG Rhythm Review – Atrial Flutter

Atrial Flutter ECG
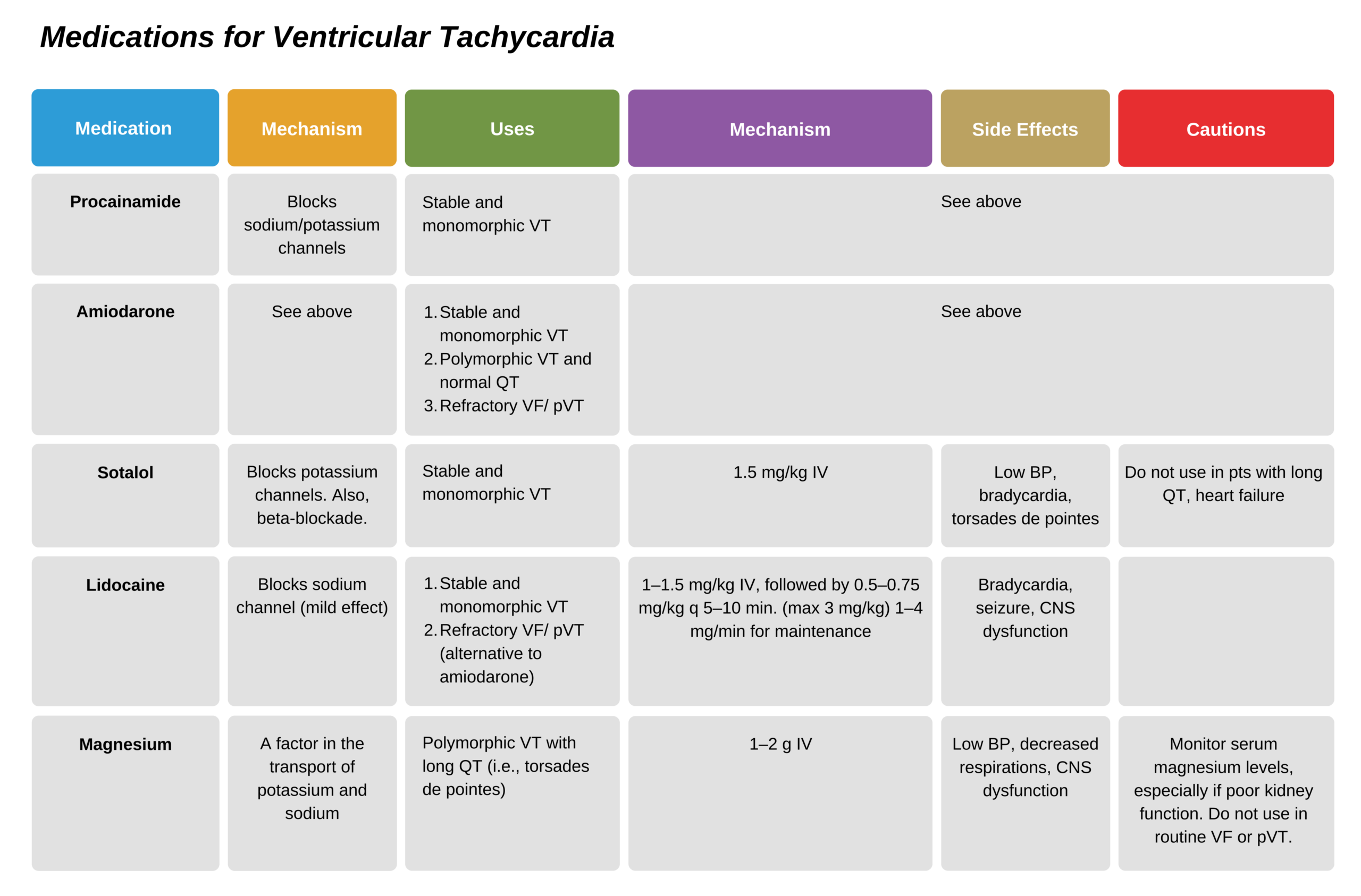
Polymorphic VT
Polymorphic or irregular VT is managed identically to VF; it requires urgent defibrillation. Medications should be used to prevent recurrence of the arrhythmia, and responders should determine the underlying cause and evaluate for long QT syndrome.
- If long QT is present: any medications that prolong the QT interval should be stopped. The patient should be evaluated for electrolyte abnormalities or other predisposing factors.
- If the patient has a familial syndrome with long QT, isoproterenol should not be used. The VT should be managed with magnesium IV, beta-blockers, or pacing.
- If this is an acquired long QT, it should be treated with IV magnesium. Pacers or isoproterenol can be added if there is bradycardia or pauses of the rhythm.
- If no long QT, it is likely associated with acute MI. Treatment is with amiodarone or beta-blockers to decrease the chance of recurrent arrhythmias. Magnesium is not recommended in these cases.
Related Video: ECG Rhythm Review – Polymorphic Ventricular Tachycardia (Torsades de Pointes)
Related Video: ECG Rhythm Review – Ventricular Tachycardia
Stable Wide QRS Tachycardia
These may originate in the ventricle or above the ventricle.
However, it is important to note:
- Wide QRS is treated as originating in the ventricle unless proven to be otherwise.
- Unstable patients with a pulse are treated with synchronized cardioversion.
- In patients with no pulse, treatment is similar to VF, i.e., defibrillation.

Supraventricular Wide QRS Tachycardia from Left Bundle Branch Block
Management: if the patient is stable, responders can try to determine the etiology to guide the direction of treatment.
- If the origin is unknown and the rhythm is regular with a monomorphic QRS, adenosine may be used and administered in the same manner as for paroxysmal SVT.
- Verapamil should not be used unless the arrhythmia has been shown to originate above the ventricle. Ventricular arrhythmias managed with verapamil can lead to significant hypotension.
- Stable patients with VT should be managed with antiarrhythmics or cardioversion. Options include amiodarone, procainamide, and sotalol. These should be used over lidocaine. Patients with long QT should not receive procainamide or sotalol.