ACS Complicated by Heart Failure or Shock
ACS complications occur and include hypotension and shock, as well as pulmonary edema, heart failure, and hypertensive emergencies. Patients may present in shock or can progress to shock. We will discuss the management of these patients as well as how to guide treatment decisions based on patient response.
Main Points
- Cardiac shock causes the most deaths in acute MI presenting to the hospital
- Cardiogenic shock prevalence and mortality remain high. 50% of patients will die.
- Cardiogenic shock involving the right ventricle carries similar mortality to that involving the left ventricle.
- Patients in this group should be managed in facilities that can provide invasive treatment, including PCI, IABP, or CABG. This may require a hospital to hospital transfers
- Patients under 75 should be managed invasively; selected patients over 75 can be managed similarly
- When shock or heart failure occur after admission, intervention with invasive therapy should occur if shock presented within 36 hours following MI onset
Key Takeaway
A routinely applied protocol should be used for all patients at risk to diagnose and manage ACS chest pain.
Heart Failure, Shock and Left Ventricular Failure
Shock indicates a significant and persistent inadequate flow of blood and oxygen to tissues and organs. While shock and hypotension are intimately linked, they are not equivalent. Shock specifically refers to inadequate oxygenation of tissue. The underlying cause of shock is not always apparent. There may be no significant hypotension. Consequently, diagnosis is usually based on:
- Critically ill appearances/ abnormal mental status
- Hypotension (under 90 mm Hg)
- Tachycardia (over 100 bpm)
- Tachypnea (respiration over 22 per minute/ PaCO2 under 32 mm Hg)
- Acidosis (elevated lactate over 4 mmol/L)
- Poor urine output (under 0.5ml/kg/h)
Diagnosing Shock
Some, not all, of these parameters will be apparent; for instance, medication may blunt some physiological responses to shock. Additionally, the time course may impact the severity of the signs. Shock can be categorized into four groups: hematological, neurological, cardiogenic, and vasogenic. Alternatively, the groups are volume, cardiac, and distributive. Finally, categorization can be based on perfusion: volume, pump, resistance, and rate
- Volume: hypovolemia (i.e., dehydration, bleeding)
- Pump: inadequate cardiac function (i.e., impaired contractility, obstruction from tamponade, PE)
- Resistance: abnormal vascular resistance or vascular distribution (i.e., sepsis)
- Rate: bradycardia, tachycardia, arrhythmias
Based on these classifications, the initial treatment strategy can be chosen:
- Hypovolemic: provide volume
- Cardiogenic: support cardiac pump function
- Distributive: vasoactive medications
- Obstructive: relieve obstruction

Fluid resuscitation treats hypovolemic shock.
Most patients will require a combination of therapies as multiple systems may fail with severe or prolonged shock. These groups of patients likely will have poor cardiac perfusion, which may result in cardiac dysfunction. This portends poor prognosis as ICU patients with elevated cardiac biomarkers, but no CAD have poor outcomes.
Evaluating Cardiac Output
Evaluation and management of cardiac output are often required in shock. The important relationships for cardiac output include:
- Arterial blood pressure = Cardiac output x Total Vasculature Resistance
- Cardiac Output = heart rate x stroke volume
Related Video: What is the Cardiac Output Formula?
Stroke volume comprises the following:
- Preload or venous return
- Afterload or Peripheral vasculature resistance
- Cardiac contractility
Related Video: What is Cardiac Output?
While cardiac function is multidimensional, volume parameters have a significant effect. With normal volume, output is optimal when the individual is at rest with not disease processes. With low volumes, venous return fails, and cardiac output decreases. The heart increases heart rate and contractility to compensate. Pulmonary arterial catheters can measure filling pressure (i.e., central venous pressures/ capillary wedge pressures) as well as cardiac output and calculate vascular resistance. Echocardiograms can also evaluate etiologies of low output or blood pressure. Using these measures, three mechanisms for shock can be determined: vasogenic, hypovolemic, and cardiogenic.
Of course, pulmonary arterial catheters are not without complications and can only help diagnose, but not treat shock. Additionally, for many patients, the evaluation of filling pressures clinically is enough to diagnose and guide treatment strategies.
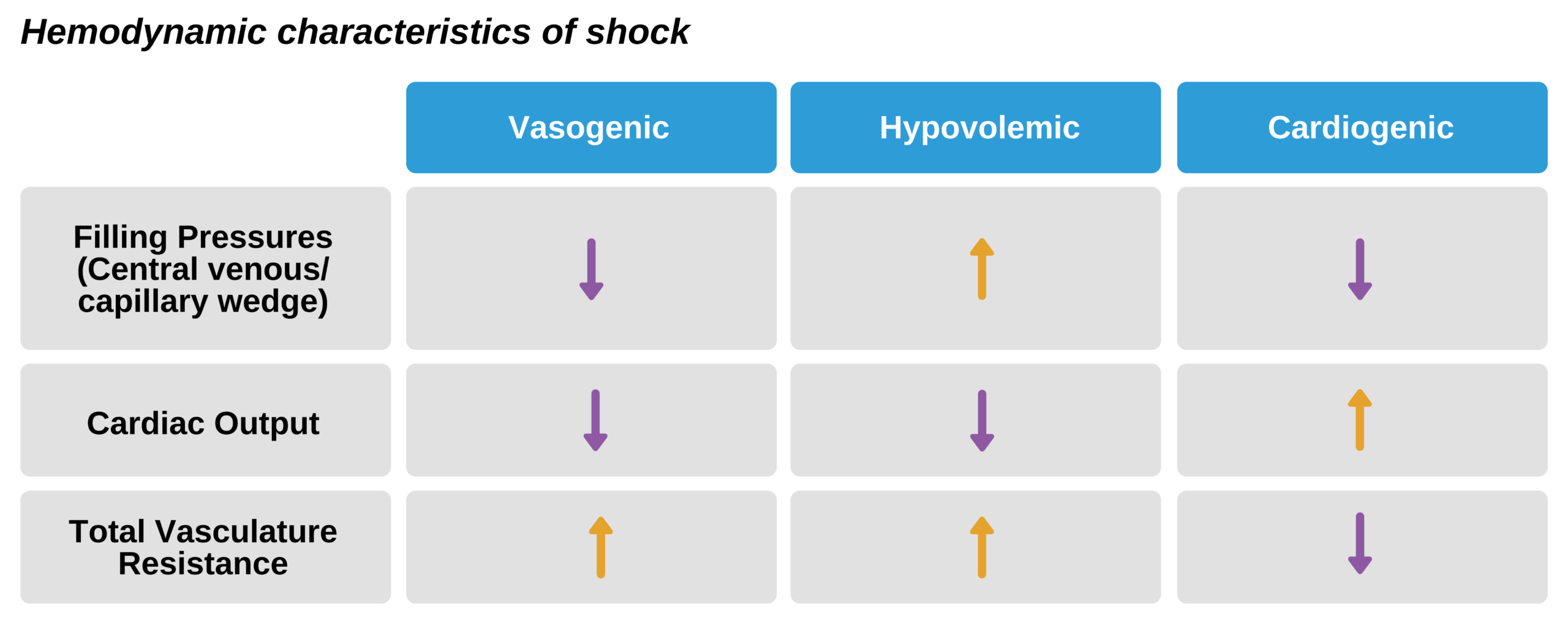
With hypovolemia filling pressures are low, leading to decreased cardiac output and the need for an increase in total vasculature resistance. In cardiogenic shock, cardiac output is low due to poor contractility, causing filling pressures to rise. Total vasculature resistance increases to compensate for poor cardiac output. In vasogenic shocks, total vascular resistance is low due to vasodilation, which leads to an associated decrease in filling pressures and a compensatory increase in cardiac output. Central venous pressure estimates the pressure of the right atrium, while capillary wedge pressures estimate pressures of the left atrium.
Cardiogenic Shock in Acute MI
When as much as 40% of the left ventricular muscle is infarcted, cardiogenic shock occurs, leading to a 60% rate of death. The incidence of such cardiogenic shock was just under 4% in 2007 (from over 5% in 1999).
Non-STEMI cardiogenic shock
Cardiogenic shock can occur in non-STEMI patients and is associated with a history of MI or left ventricular dysfunction. Mortality can be as high as in patients with large acute MI due to a delay in the diagnosis as well as significant patient comorbidity. IT is important to know that non-STEMI patients tend to be older with more significant cardiac disease, including heart failure, history of MI, and multiple vessel disease than STEMI patients. ECG may not identify abnormalities in the region of the circumflex artery, which may cause as many as 1/3 of cases of cardiogenic shock.
Cardiogenic Shock mechanisms
Acute MI can lead to vascular instability and heart failure. Cardiogenic shock is the resultant shock that occurs following cardiac muscle failure due to a catastrophic heart attack. As cardiac output drops, the heart rate attempts to increase to compensate for associated reduced stroke volume. However, due to the failure of cardiac muscle, the ventricle becomes dilated. It is unable to maintain an adequate ejection fraction with contractions.
Beta-blockers in heart failure
While an increase in heart rate is a physiologic response to improve cardiac output, the rapid rate requires oxygen consumption, something that ischemic tissue lacks. Consequently, tachycardia can increase ischemia in the tissue and extend the infarct size. Beta-blockers can aid in ischemia by decreasing adrenergic excess, reducing oxygen need, and limiting infarct size, particularly if there is a large anterior infarct with no associated heart failure. However, Beta-blockers should not be used in cardiogenic shock when tachycardia is relied upon for life-sustaining cardiac output.
Hemodynamics in Cardiogenic Shock
Increased left ventricular pressure (over 25-30 mm Hg) causes pulmonary edema with the same pressure change in the right ventricle cause edema of the periphery. Low cardiac output will cause increase adrenergic stimulation to help compensate with tachycardia and peripheral vascular resistance to maintain flow to the heart and brain. The heart “sees” a higher afterload, which can limit left ventricle ejection. In this case, cardiac output falls, and the patient develops hypotension and acidemia. In combination with pulmonary edema, this signals cardiogenic shock.
Patients with left ventricular dysfunction can have signs of poor perfusion. The cardiac index, which is cardiac output with a correction factor for the bodily surface area, is under 2.2 L/min. Additionally, volume refractory hypotension exists for at least one hour, and capillary wedge pressure is over 18 mm Hg.
Effecting change in Cardiogenic Shock
Cardiogenic shock causes the majority of death in hospitalized patients with acute MI. while it is classically thought that poor cardiac output always leads to peripheral vasoconstriction, research indicates that a subgroup may actually have low vascular resistance. These patients may experience inflammation that inappropriately blocks the compensatory vasoconstrictive response. More research is needed to determine the best way to manage these patients.

Cardiogenic Shock Paradigm
Managing Cardiogenic Shock in acute MI
The 50% death rate associated with cardiogenic shock from MI is common in the first 48 hours. Initial management involves oxygen, IV nitrates, and diuretics. Morphine can be used for chest pain but should be done cautiously. Hypotension with systolic BP under 100 mm Hg indicates the cautious use of nitrates and morphine.
In contrast, systolic BP under 90 mm Hg precludes their use. With severe hypotension, all vasodilators must be stopped, and vasopressors added. If this is not successful, advanced vascular monitoring is required. Advanced invasive interventions are indicated at this point. Intra-aortic balloon counterpulsation to assist circulation may be used in specific patient populations. Multiple research studies indicate that PCI is preferred in this patient population than fibrinolytic treatment. These studies conclude decreased mortality and increased survival in cardiogenic shock with PCI, CABG (and associated IABP) compared to fibrinolytics

Cardiogenic Shock Management
A randomized and controlled study, known as the SHOCK trial, evaluated the best time and method for revascularization in cardiogenic shock. The findings indicated that IABP and PCI or CABG were superior to fibrinolysis at 6 months to one year with reduced mortality. Recent follow-up shows that 2/3 of patients surviving to discharge and managed with invasive therapy were still alive at 6 years. The research indicated that any patient with acute MI, concern for shock, left ventricular dysfunction, pulmonary edema, heart failure, or other high-risk signs should be managed in a facility capable of performing invasive revascularization. The 2004 ACC and AHA updated the guidelines for shock management in ACS in patients under 75. The recommendations were upheld in 2010 at the international consensus conference:
Triage patients to facilities that have invasive intervention capabilities
- Provide PCI for STEMI patients with shock/significant heart failure regardless of a delay from onset of MI symptoms
- Perform angiography with a plan for revascularization in STEMI patients with shock/significant heart failure developing following presentation.
- Provide emergency PCI or CABG in STEMI patients with cardiogenic shock regardless of a delay from onset of MI symptoms
- Perform PCI of a significant stenotic artery in ACS patients with shock/significant heart failure when anatomically able
- Administer fibrinolysis in patients with STEMI with cardiogenic shock when they cannot receive invasive revascularization
- Consider IABP counterpulsation in STEMI patients who develop cardiogenic shock and remain unstable following medical therapy.
- Provide emergency CABG in STEMI patients with persistent ischemia, shock, heart failure and other high-risk findings who are not candidates for PCI
- Consider left ventricular assistant devices in patients with cardiogenic shock refractory to non-invasive therapy.
- If there are contraindications to fibrinolytic therapy (based on the fibrinolytic checklist), transfer to a hospital capable of invasive revascularization may be appropriate
Right Ventricle Shock
In most patients, the inferior wall of the heart and right ventricle are supplied by the right coronary artery (RCA). If an obstruction occurs in this artery, RV ischemia, and possible infarct, can occur. 1/3 of patients with an inferior MI will have involvement of the right marginal branch of the RCA, and half of these will have a hemodynamically unstable result. The hemodynamic infarct doubles the mortality of an otherwise more favorable area of disease. The right ventricle is somewhat resistant to infarct, and ischemic tissue can recover.
The SHOCK trial found that RV shock associated with acute MI occurs in younger, healthier patients with lower rates of prior MI or multiple vessel disease. Unfortunately, the mortality rate was surprisingly as high as patients with LV shock associated with acute MI. The likely reason was that right ventricle dysfunction led to pulmonary compromise and back up of the left heart. As a result, left ventricular dysfunction is caused by the right ventricle dysfunction. When infarct of the inferior wall is found, right ventricle dysfunction may be a cofactor, and a 12 lead ECG with right-sided placement should be obtained. Finding of 1mm ST elevation V4R lead is indicative of this diagnosis.

Right Coronary Artery Anatomy

Inferior Wall MI ECG
Signs for right versus left ventricle shock are different. With shock from the right ventricle, the lung sounds are clear, and jugular veins are distended due to increased pressure in the right atrium. However, the three findings of hypotension, clear lung, and distended jugular veins are present in only 25% of patients.
While both forms of shock are treated with emergency reperfusion, associated medical care differs. Poor right ventricle function must be managed by maintaining preload for right heart filling. Medications that worsen preload, such as morphine, diuretics, nitrates, and ACEI, can decrease survival and are not indicated. Instead, careful volume administration is indicated. Provide boluses of 250-500ml incrementally with close monitoring of vitals. If fluid resuscitation is ineffective, patients may require ionotropic stimulation with dobutamine and possibly the addition of dopamine. If there is associated multiple vessel disease or history of MI, left ventricle dysfunction may require IABP.
Treating infarct of the Right Ventricle
As noted above, in infarcts of the inferior wall, a 12 lead ECG with right-sided placement should be obtained. Finding of 1mm ST elevation V4R lead is indicative of this diagnosis. Infarct of the right ventricle causes up to 30% mortality, and consequently, patients are candidates for reperfusion. Fibrinolytics can be administered to treat the right ventricle dysfunction. PCI should be used for those in shock. Never administer medications that will adversely affect preload, including ACEI, nitrates, and diuretics.
ACS with Pulmonary Edema or Shock
Both pulmonary edema and shock are emergent issues. Shock causes unacceptable perfusion of the tissues resulting in weak pulses, poor urine output, cold extremities, poor capillary output, and acidemia. Heart failure can lead to pulmonary edema with resultant tachypnea, rales on lung exam, respiratory distress, hypoxemia, frothy sputum, and cyanosis.
Related Video: What is Pulmonary Edema?
Initial management
For pulmonary edema, initial management when hypotension/shock are excluded
- Oxygen (with positive pressure if needed)
- Nitroglycerine
- Diuresis
- Morphine
Patients should be seated upright with legs dangling if not hypotensive. This will expand the lungs, decrease breathing work, and minimize venous return. Morphine further causes venous dilation and decreases both pre- and afterload. Ensure IV access and monitor cardiac status. Ensure good oxygen saturation with supplementation and oximetry. Check laboratory evaluation to evaluate comorbidities or complications.

Complex STEMI Acute Management
Oxygenation
Provide high flow oxygen, initially at 5-6 L/min, using a mask. Options include nonrebreathers due to high oxygen concentration or bag-masks to aid with ventilation. Additionally, continuing positive airway pressures can be helpful. If there is respiratory distress or impending failure, intubate the patient. Need for intubation is indicated by:
- Inadequate PaO2 below 60 mmHg on 100% oxygen
- Altered mental status indicating brain hypoxia
- Increasing PCO2
- Respiratory acidosis
Ensure intubation is successful using waveform capnography and confirm by checking breath sounds, chest rise, and other clinical signs.
Nitroglycerin
IV nitroglycerin should be given to patients in pulmonary edema as long as they are not hypotensive or in shock. The medication improves congestion via vasodilation and improves preload. It also decreases total vascular resistance, which improves cardiac output. An alternative to IV route includes sublingual or spray.
Diuresis
Diuresis is vital for pulmonary edema. Loop diuretics like furosemide, initially lower venous tone and improve capacitance. This decreases left ventricle preload and can improve symptoms. Next, it causes diuresis in about 5-10 minutes. Start with a dose of 0.5-1mg/kg over 1-2 minutes in furosemide naïve patients. Repeat with 2 mg/kg dose after 20 minutes if needed. In patients who already use furosemide, simply double their prescribed dose. In patients with massive fluid retention, refractory heart failure, or kidney disease, doses may need to be increased.
Nesiritide
This is an analog to the brain natriuretic peptide (BNP) and is useful in decompensated heart failure. It has been shown to augment hemodynamics, improve dyspnea and clinical status.
Morphine
Morphine causes vasodilation, which decreases preload. Similarly, it decreases afterload via arterial dilation. Recent data suggest that it may not be as effective as ACEI, and consequently, it is not considered primary therapy.
Improving Blood Pressure
Pulmonary edema is often complicated by hypertension. This is due to comorbid hypertension, as well as the associated adrenergic excess. While pulmonary edema can improve hypertension, initial management can also be effective. Nitroglycerin can be used to manage hypertension due to its effects on preload as well as afterload. The goal is to decrease systolic BP up to 30 mm Hg. IV nitroglycerin at 10mcg/kg is a good starting dose an can be increased to achieve the goal. Ensure no significant hypotension leading to inadequate perfusion.
Secondary treatments
- Dopamine for systolic BP between 70-100 mm HG with shock
- Dobutamine for systolic BP between 70-100 mm HG without shock
- ACEI for systolic BP over 100 mm Hg but not at goal target of 30 mmHg below initial BP
These treatments are only used as second-line for adequate BP response.
Patient is not hypotensive but the BP is not adequately controlled
- Administer ACEI to lower afterload and improve left ventricle recovery following STEMI
- Consider continuing nitrates. Note that tolerance to the BP effect can occur after 24 hours, so choosing another medication may be necessary
- IV nitroglycerin at 10 mcg/min. Use nonabsorbable tubing. Increase 5-10 mg q 3-5 minutes to achieve a response. Increase as much as 20 mcg/min until adequate response. Remember to titrate down the dose when the goal is reached. when normotensive, the goal is 10% of initial BP, when hypertensive, the goal is 30 mm Hg below initial BP
Patient with Systolic BP 70-100mm Hg
The clinical signs are important here. If shock is evident, administer dopamine IV; if shock is not evident, infuse dobutamine IV.
Additional Treatments
Note that other competing factors should be assessed and managed concurrently. For instance, if there is concomitant STEMI with pulmonary edema, reperfusion should be pursued. Other evaluations, such as ECG for diagnosis and evaluation for reversible causes, should not be delayed. Additionally, echocardiograms for bedside assessment can be useful for diagnosis and to guide treatment. Finally, early transport to facilities with interventional revascularization capabilities should be completed.