Algorithm for Bradycardia with Pulse

Adult Bradycardia With Pulse Algorithm
Once responders have identified the rhythm as bradycardia, the algorithm should be used as a guide to tailor therapy to the individual patient.
Box 1: Identification of Bradycardia
Bradycardias are heart rates < 60 beats per minute. When symptoms arise, the rate has usually fallen to < 50 beats per minute, and this is the working definition of bradycardia in the AHA algorithm.
Box 2: Identifying and Treating the Underlying Cause
Bradycardia causes a significant decrease in cardiac output, which leads to the signs and symptoms associated with bradyarrhythmias. It is vital to identify symptomatic bradycardia and begin treatment.
The provider must ensure that the patient’s airway is patent and administer oxygen if hypoxemic. The team monitors oxygen saturation continuously.
Cardiac monitoring should be initiated to identify the rhythm. It is essential to obtain IV or IO access for fluid and medication therapy. The team monitors the patient’s blood pressure and obtains a 12-lead ECG if that does not delay therapy.
Box 3: Bradycardia with Symptoms?
Untreated symptomatic bradycardia can lead to cardiac arrest. The provider assesses for signs and symptoms of hemodynamic instability, including:
- Altered mentation
- Hypotension
- Signs of shock
- Chest discomfort
- Heart failure
If the patient is hemodynamically stable, the team proceeds to Box 4; if hemodynamically unstable, they proceed to Box 5.
Box 4: Treatment of Asymptomatic Bradycardia
If the patient has no severe signs and symptoms associated with bradycardia, the team continues to monitor and observe. Continuous reassessment is essential, as the patient’s condition may deteriorate.
Box 5: Treatment of Symptomatic Bradycardia
Medication, electrolyte imbalance, or myocardial disease secondary to acute myocardial infarction can cause atrioventricular blocks. It is critical for the provider to determine if the symptoms are caused by the bradycardia. If they are not, the provider treats the underlying cause.
Key Takeaway
The most important question before treating bradycardia is whether the patient’s symptoms are caused by the bradycardia or some other issue.
Box 6: Further Considerations
The provider considers expert consultations and transvenous pacing if symptomatic bradycardia persists.
Variations of Bradycardia
While most define bradycardia as a heart rate below 60 beats per minute, there are some individuals in whom this heart rate is physiological. For example, professional athletes or patients who take beta-blocker medications may have a resting heart rate below 60 that allows adequate perfusion. These patients do not necessarily need treatment.
On the other hand, another individual may have a heart rate over 60 beats per minute that is inappropriate for their condition and inadequate for systemic perfusion. This can occur in a hypotensive or septic patient whose condition would require a relative tachycardia to allow adequate perfusion. These patients may require treatment for symptomatic relative bradycardia, either via management of the underlying condition or with chronotropic medications or pacing if the bradycardia is causing instability.
Symptoms of Bradycardia
Bradycardia only needs to be treated if it is the cause of a patient’s symptoms. Since heart rate is a significant component of cardiac output (remember that CO = HR x SV), unless stroke volume increases proportionally, a slower heart rate will lead to a drop in the cardiac output, which can result in symptoms.
On the other hand, cardiac output may be decreased due to low stroke volume (perhaps from hypovolemia) rather than bradycardia. In this case, the provider should treat the underlying cause, hypovolemia, to manage the symptoms.
Bradycardia symptoms include:
- Low blood pressure
- Decreased or altered mental state
- Shock
- Ischemic chest pain
- Heart failure
Types of bradycardia
- Sinus bradycardia
- Atrioventricular (AV) heart block
- 1st-degree block
- 2nd-degree block
- Type I (Mobitz I or Wenckebach)
- Type II (Mobitz II)
- 3rd-degree (complete) block
Sinus bradycardia is due to slowed sinus electrical activity. Generally, the atrial and ventricular rates are equivalent, and consequently, slowed sinus activity will cause slowed ventricular contraction. On the other hand, if there is an atrioventricular (AV) heart block, the atrial rate may not correlate with the ventricular rate, so that the atria may beat at a normal rate with a bradycardic ventricular rate.
There are three major classifications of AV block: 1st, 2nd, and 3rd (or complete). AV block may be due to abnormal electrolytes, medications, or anatomical abnormalities of the heart due to infarct, infection, or other causes. AV blocks are a major cause of bradycardias, and the type of AV block can help guide treatment.
Generally, 2nd- and 3rd-degree blocks are more clinically significant and more likely to cause symptoms. A 3rd-degree (complete) AV block is most likely to lead to cardiac arrest and usually requires immediate intervention with pacing. It is more important to recognize AV blocks as the cause of symptomatic bradycardia than to determine their classification.
Managing Bradycardia Causing Poor Perfusion
Points to Remember
- The initial management of symptomatic or unstable bradycardia is atropine. (Class IIa, Evidence level B)
- Atropine may not be effective in patients with Mobitz II 2nd-degree or 3rd-degree AV block. Rather, these patients should be managed with transcutaneous pacing or beta-adrenergic medications. However, Wenckebach or Mobitz I AV 2nd-degree AV block can be treated with atropine, which helps to reduce vagal activity.
- Clinicians should be cautious about using atropine in patients with acute coronary syndromes as it may increase heart rate and oxygen requirements, which can worsen cardiac ischemia.
- Transcutaneous pacing can be utilized as second-line management for symptomatic/unstable bradycardia that has failed atropine.
- Epinephrine and dopamine may also be used in bradycardia when atropine is ineffective. Providers should not use isoproterenol and dobutamine due to the side effects of ventricular arrhythmia (isoproterenol) and hypotension (dobutamine).
- Medications and transcutaneous pacing should not be used long-term for the management of bradycardia. Instead, patients should be transitioned to transvenous pacing. (Class IIa, Evidence level C)
In the algorithm for bradycardia with a pulse, treatments are listed according to increasingly critical conditions. For patients with unstable bradycardia that is at risk for progressing to cardiac arrest, interventions should be performed concurrently, including rapid treatment with atropine, easy access to transcutaneous pacing, and dopamine or epinephrine as needed.
Atropine
The vagus nerve innervates both the sinus and the AV nodes, effectively slowing down electrical conduction and heart rate when activated. Vagal nerve endings release acetylcholine, which mediates these effects. Atropine acts as an antagonist, blocking acetylcholine effects and increasing heart rate and electrical conduction. Therefore, atropine is the preferred treatment for symptomatic bradycardia and blockage at the AV node and can be used as a temporary measure until pacing is available.
Key Takeaway
Never allow the delivery of atropine to delay use of transcutaneous pacing or beta-adrenergic medications in patients progressing to cardiac arrest.
Research indicates the benefit of IV or IO atropine dosage of a 1.0 mg bolus repeated at 3- to 5-minute intervals. ACLS recommends a total dose of IV atropine up to 3 mg.

Atropine for Injection
As previously noted, atropine is not effective for patients with Mobitz II 2nd-degree or 3rd-degree blocks, and pacing or beta-adrenergic medications should be used for these patients instead. Additionally, if the patient is unstable and progressing towards arrest, it is recommended to preferentially treat with beta-adrenergic medications or pacing rather than delay their administration by giving atropine.
Note that patients with heart transplants do not respond to atropine as these hearts no longer are innervated by the vagus nerve. In patients following heart transplant, paradoxical bradycardia has been noted with atropine use during anesthesia. In addition, it is rare but possible for VF or VT to be an outcome of atropine administration.
Related Video: Atropine – ACLS Drugs
Transcutaneous Pacing (TCP)
TCP is the necessary next step in those patients who are unresponsive to atropine. The clinician ensures the patient tolerates this procedure and checks for electrical capture and adequate mechanical function. TCP may be painful, so adequate analgesics or sedation must be administered, but it should be noted that certain sedatives can negatively affect the cardiac rhythm.
TCP does not always result in adequate ventricular contractions, so the pulse and signs of perfusion need to be closely monitored. The next step will likely be transvenous pacing, and thus cardiac consultation and preparation are necessary steps.
Many defibrillators can concurrently provide TCP, making this a quick next step for the appropriate patient. As TCP only requires placement of electrical leads on the skin, the team can provide this treatment at the bedside.
Related Video: Transcutaneous Pacing
Second-line agents for Bradycardia
There are other medications used as second-line agents for bradycardia. These include the beta-adrenergic medications, epinephrine and dopamine, in cases when atropine is not effective. These medications are utilized temporarily until pacing can begin. They are also used in the case of specific drug overdoses like beta-blocker or calcium channel blocking medications.
Epinephrine
Epinephrine for bradycardia is given as an infusion of 2–10 mcg/min and adjusted to ensure adequate vital signs. As epinephrine leads to vasoconstriction, clinicians must ensure that the patient has adequate vascular volume or provide fluid resuscitation as needed.
Dopamine
Dopamine is especially useful for symptomatic bradycardia in which the patient is hypotensive after atropine has already failed. The dose is 5–20 mcg/kg each minute and adjusted to the patient’s vital signs and response. Dopamine can cause dilation of the splanchnic vasculature and symptomatic hypotension when given at low doses. Consequently, clinicians must ensure adequate vascular volume or provide fluid resuscitation as needed.
Diagnosing and Treating Bradycardias
Sinus Bradycardia
Since sinus bradycardia is a sinus rhythm with a pace below 60 beats per minute, the rhythm will have normal P waves originating from the sinoatrial node (upright in leads aVF, I, II, and III).
The P waves in sinus rhythm reflect the electrical activity in the atrium rather than AV node conduction or the response of the ventricle. Those should be evaluated by assessing the PR interval and the QRS morphology.
Sinus bradycardia can have other etiologies. For example, patients on beta-blockers, vagal stimulation, and high exercise tolerance from physical conditioning can all cause this rhythm, and treatment is not necessarily indicated. Inferior MI can be a pathologic cause.
Related Video: ECG Rhythm Review – Sinus Bradycardia
Pathophysiology
- Sinus bradycardia is due to slowed sinoatrial electrical impulses.
- It is often a response to an underlying concern rather than a primary condition.
ECG Findings
Symptoms and Signs of Bradycardia
- Often asymptomatic during rest
- Increasing symptomatology with increasing activity
- Symptomatology includes:
- Dyspnea
- Dizziness
- Fatigue
- Syncope
- Signs include
- Diaphoresis
- Hypotension
- Pulmonary congestion and pulmonary edema
- Other ECG findings can be superimposed on sinus bradycardia, such as ST segment changes, T wave abnormalities, and abnormal ventricular rhythms.
- With increasing bradycardia, the QT interval lengthens, and accurate measurements will require an adjustment for the heart rate.
Underlying causes
- It is normal to see unusually slow heart rates in physiologically trained individuals. Additionally, the heart rate decreases with age and sleep.
- It can be due to vagal stimulation, such as vasovagal response, including Valsalva, rectal stimulation, emesis, and carotid sinus massage.
- It can be caused by ACS involving the right coronary arteries (RCA), as these often supply the sinoatrial node.
- A range of medications can affect the sinus node, including beta-blockers, calcium channel blockers, amiodarone, quinidine, and digoxin.
Management
- Asymptomatic and even mildly symptomatic bradycardia does not necessarily require treatment.
- If the patient has significant symptoms affecting perfusion, clinicians should follow the algorithm for bradycardia with a pulse.
- Attempts should be made to determine the underlying cause, such as ACS or hypoxia, and manage this.
- Supportive care is important to continue while managing the condition and can include providing oxygen in cases of hypoxia.
Atrioventricular (AV) Heart Block
Abnormal conduction between the atrium and ventricle causes the AV heart blocks. This can originate at any location in the tract conducting impulses between the two compartments and can arise slowly or suddenly. It is vital to understand the electrical pathways, their physiology, and underlying associated comorbidities to appropriately manage and treat AV blocks.
- Anatomical conduction pathway lesions (e.g., infarct, calcium deposition, fibrosis)
- Increased vagal response (e.g., inferior infarct, carotid sinus reactivity, enhanced visceral stimulation)
- Slowed conduction or a longer refractory period (often related to medications)
- Physiological blockade due to increased atrial rate. This is a normal response that serves to prevent excessive ventricular rates. Such a manifestation is the 2:1 AV heart block seen in conditions such as atrial flutter with atrial rates > 300 beats each minute. Note that at normal atrial rates, AV blockade is not physiological.
Key Takeaway
Cardiac disease is the primary cause of death all over the world, causing over 17 million premature deaths. Awareness and education are needed to prevent and treat heart disease.
Understanding (AV) Heart Block
AV block is categorized based on the site or degree of blockage. The AV node is a complex system of fibers located at the base of the right atrium, close to the tricuspid valves, and anterior to the coronary sinus ostium. Conduction speed is normally a little slower at the AV node, and the normal PR interval is 0.20 seconds or less. The bundle of His, the outflow tract of the AV node, then penetrates through the annulus ring to enter the intraventricular septum. The fibers then divide into the right and left bundle branches.
Related Video: Cardiac Action Potential Part 2: Role of the AV Node

Heart’s AV Node and Conduction Pathway
Related Video: Conduction System of the Heart Part 1: Basics of Conduction
Related Video: Conduction System of the Heart Part 2: Back-Up Pacemakers
Related Video: Conduction System of the Heart Part 3: Relating to an ECG
Site
- AV blocks can occur superior to or at the AV node, referred to as supranodal and intranodal, respectively. Together, these are categorized as nodal blocks.
- An AV blockage inferior to the AV node is categorized as an infranodal block.
The site of the blockage can help determine the underlying pathology, management, and prognosis.
Degree
- 1st
- 2nd (Mobitz I or II): often further classified by the ratio between atrial and ventricular contractions
- 3rd (Complete)
1st-degree AV Block
1st-degree block is technically a slowed transit of electrical activity between the atrium and ventricle. Consequently, it is defined by a prolonged PR interval. The delay usually occurs at the AV node but can occur anywhere from the node to the right or left bundle branch.

1st-Degree AV Block ECG
Pathophysiology in 1st-degree Block
- usually has a slowed conduction at the AV node and thus a prolonged but stable PR interval
- is generally asymptomatic and a normal variant that usually does not require treatment
- may be due to medications or increased vagal activity
Related Video: One Quick Question: What are the First-Degree Heart Block Criteria?
ECG Findings
Symptoms and Signs of 1st-degree Block
It is generally asymptomatic.
Underlying Causes
- It can be due to vagal stimulation, from vasovagal responses including Valsalva, rectal stimulation, emesis, and carotid sinus massage.
- It can be due to a range of medications that affect AV node conduction. Such medications include beta-blockers, calcium channel blockers, and digoxin.
- It can be associated with increasing age and certain diseases.
- It can be due to ACS involving the right coronary artery (RCA) as it often supplies blood flow to the AV node.
Management
- Generally, no treatment is required as patients are symptomatic. If the patient has symptoms, there may be another cause.
- A new-onset 1st-degree block may progress to 2nd-degree block in certain settings such as underlying medical illness. Clinicians should monitor for this and ensure adequate oxygenation of at least 94% saturation.
- 1st-degree blocks that progress to symptomatic higher degree blocks should be treated using the algorithm for bradycardia with a pulse.
2nd-degree AV Block (Mobitz/Type I)
2nd-degree block is intermittent, with some electrical activity making it through the conduction system while others do not. There are two types:
- Mobitz (Type) I or Wenckebach
- Mobitz (Type) II
Type I 2nd-degree block usually occurs at the AV node. The PR interval is progressively prolonged until one sinus impulse is completely blocked. After this, the pattern repeats. It is usually described by the P:QRS ratio, indicating the number of P waves to each QRS complex. If the ratio is 2:3, then every third P wave does not have a QRS complex following it.

2nd-Degree AV Block, Mobitz Type I ECG
Related Video: ECG Rhythm Review – Second-Degree Type 1 Heart Block (Wenckebach)
Pathophysiology
This arrhythmia occurs at the AV node. Prolonging of the PR interval is normal at rapid atrial rates but is abnormal when the atrial rate is within normal limits. When this happens, it becomes Mobitz I.
Mobitz I is less concerning than Mobitz II because it is usually generated at the level of the AV node rather than more distally in the conduction pathway (as is the case of Mobitz II). Even in worsening cases (more dropped ventricular beats), the ventricular rate is typically faster and more likely to allow for adequate systemic perfusion.
Symptoms generally occur with higher grade blocks (or increasingly dropped beats). When there is a blockage in the conduction pathway, QRS complexes are independently generated from locations distal to the blockage. The lower the site producing independent QRS complexes, the more likely they will be abnormal, erratic, and inadequate for perfusion. Thus in Mobitz I blocks, which occur more proximally, the independently produced QRS is more likely to be adequate.
Most commonly, Mobitz I is due to increased vagal activity, but it can also be secondary to ischemia in the area of the AV node.
The slowed activity through the conduction pathway manifests on the ECG with prolonging of the PR interval until the conduction system fails and an impulse is blocked, leading to the dropped QRS or beat. Following this, the pattern usually repeats, with conduction progressively slowing until the next dropped beat.
- There is a range of P:QRS ratios for Mobitz I.
- The P:QRS ratio can be stable or variable.
- Mobitz I is often transient and usually resolves once the underlying cause is treated.
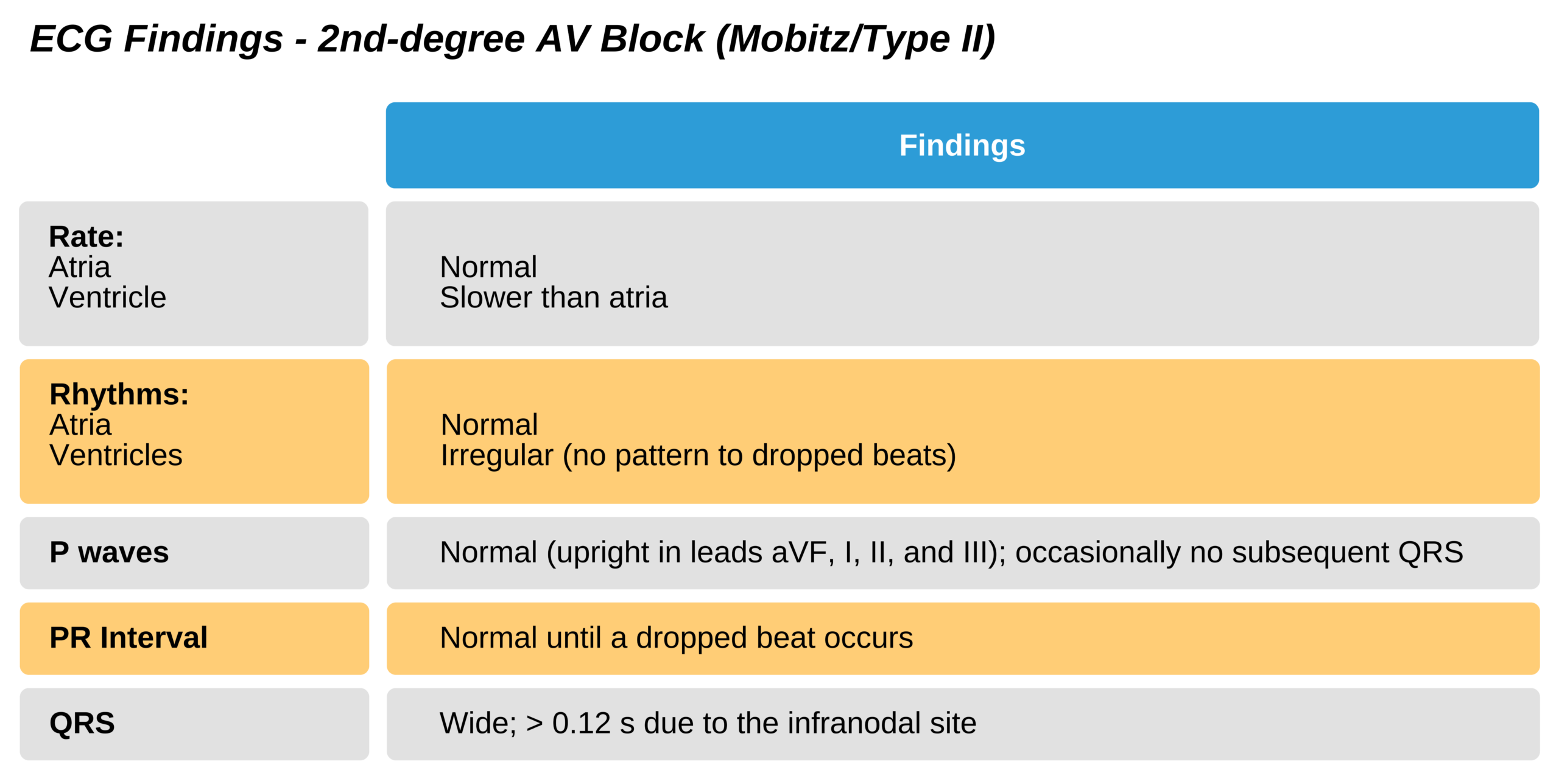
2nd-degree AV Block (Mobitz/Type II)
Type II 2nd-degree block usually occurs infranodally, either at the bundle of His or the left or right bundle branch. Unlike Mobitz I, the PR interval does not progressively prolong; instead, a random QRS is dropped. There may be no pattern to this, and multiple beats may be dropped in rapid succession.

2nd-degree AV Block, Mobitz Type II ECG
Related Video: ECG Rhythm Review – Second-Degree Heart Block (Type 2)
Pathophysiology
- This blockage takes place at an infranodal site, below the AV node. Thus there is no typical pattern for the blocked conduction. Rather, the complete block is random. This is because the bundle of His and His Purkinje fibers respond with an “all or nothing” phenomenon so that, rather than slowing conduction, conduction will either pass or not pass through.
- Due to the lower site of blockage, Mobitz II has a worse prognosis. Additionally, the ventricle rate is slower, unpredictable, and more likely to be inadequate for generating adequate perfusion.
ECG Findings
There is a characteristic stable PR interval length with intermittent dropped QRS complexes.
Symptoms and Signs of Mobitz II
Symptoms include:
- Chest discomfort
- Dyspnea
- Decreased level of consciousness
Signs include:
- Hypotension/shock
- Pulmonary congestion
- Heart failure
- ST segment changes
Underlying causes
- It is usually due to an anatomical conduction pathway lesion.
- A newly occurring Mobitz II is more likely due to a left coronary artery occlusion resulting from an ACS. Typically, the blockage is in a septal branch of the left anterior descending (LAD) artery. Such occlusions may also cause bundle branch blocks.
- Unlike lower degree AV blocks, Mobitz II is less likely to be due to increased vagal tone.
Management
Typically, Mobitz II is symptomatic and should be treated according to the algorithm for bradycardia with a pulse. Additionally, in these patients:
- cardiac consultation should be obtained
- preparations for transvenous pacing should be initiated
While atropine is usually used for bradycardia, it may not be effective in patients with Mobitz II 2nd-degree or 3rd-degree AV block. This is because these blocks occur below the AV node, where atropine is inactive. Additionally, there can be a paradoxical response to atropine with worsening of a high-grade block. Atropine increases the rate of both the sinus and AV nodes, which may lead to more impulses reaching the already damaged infranodal blockage site and cause worsening function.
Mobitz II is managed with TCP or beta-adrenergic medications as a temporary treatment until transvenous pacing is available. Clinicians ensure the patient is tolerant of this procedure, check for electrical capture, and monitor for adequate mechanical function. TCP may be painful, so the administration of adequate analgesics or sedation is required. Specific sedatives can negatively affect the cardiac rhythm.
If TCP is not available, the patient is treated with:
- Dopamine 5–20 mcg/kg/min IV
- Epinephrine 2–10 mcg/min IV
Related Video: One Quick Question: What are the Second-Degree Heart Block Criteria?
3rd-degree AV Block
3rd-degree AV block arises due to significant damage to the conduction pathway that does not allow impulses to be conducted from the atrium to the ventricle. Therefore, the atria contract more rapidly than the ventricles without any relationship between the independent compartments, which represents a complete block between the atria and ventricles. This can happen in two instances: 1) 3rd-degree or complete heart block, and 2) an underlying ventricular arrhythmia (e.g., VT) in which abnormal electrical activity arises outside of the normal conduction pathway.

3rd-Degree AV Block ECG
Pathophysiology
- 3rd-degree (complete) AV block is a total disassociation between the atria and ventricles so that there is no electrical connection between the two. The rates of the different compartments are completely independent. There is generally no connection backward (i.e., from ventricle to atrium) as well.
- The ventricular rate during 3rd-degree AV block is secondary to escape beats that are independent of the AV node. The ECG pattern of the QRS complex can provide information as to the site of the block. A narrow QRS will be initiated higher in the conduction pathway than a wider QRS.
- 3rd-degree heart block may occur in a few locations throughout the conduction pathway, and the site of pathology can help guide treatment as well as prognosis:
- AV nodal block: also termed high, junctional, or nodal block. At this proximal site, the ventricular escape pacemaker allows a more stable ventricular rate between 40 and 60 beats per minute. The QRS depolarizes normally and will be narrow because it arises proximal to the bundle of His division. Consequently, it is more likely to be temporary and has a better prognosis.
- Infranodal block: At this distal site, the escape pacemaker arises at the bundle of His or lower and suggests significant conduction pathway disease. The rhythm from this distal site is usually slower than 40 beats per minute and is unstable, leading to a wide QRS. Additionally, conduction may not occur at all, leading to asystole of the ventricles. A new-onset infranodal 3rd-degree block usually is associated with a significant anterior wall MI.
- 3rd-degree AV block can occur in conjunction with any atrial rhythm or arrhythmia. However, we will primarily discuss AV blocks associated with a sinus rhythm.
Related Video: ECG Rhythm Review – Third-Degree Heart Block
ECG Findings
Symptoms and Signs of 3rd-degree AV Block
Symptoms are usually present and include:
- Chest pain
- Dyspnea
- Decreased level of consciousness
- Syncope
Signs occasionally occur, including:
- Hypotension/shock
- Pulmonary congestion
- Heart failure
- Angina/acute MI
Underlying Causes
- Narrow QRS 3rd-degree heart block occurs at the AV node and is likely due to junctional escape rhythms. This can be caused by increased vagal tone, inferior wall ischemia, toxins (e.g., digitalis or beta-blockers), or AV nodal injury. A wide escape rhythm (> 0.12 seconds) with a slow rate (< 40 bpm) has a worse prognosis. It is more likely arising from a more distal location in the conduction pathway.
- Wide QRS 3rd-degree block is more likely due to a left coronary artery occlusion due to ACS. Typically, the blockage is in a septal branch in the left anterior descending (LAD) artery. Such occlusions may also cause blocks in the associated bundle branches.
Management
New-onset 3rd-degree heart block should be managed with transvenous pacing, especially if it has a wide QRS.
Key Takeaway
Consider transcutaneous pacing in a patient with new-onset type II 2nd-degree or 3rd-degree AV block (especially with wide QRS) in a patient with ACS.
Do not administer amiodarone or lidocaine to patients with 2nd- or 3rd-degree AV blocks.
The treatment should be initiated according to the algorithm for bradycardia with a pulse. Atropine 0.5 mg at 3- to 5-minute intervals up to 3 g total is still the drug of choice for narrow QRS 3rd-degree block or those thought to arise from the AV node.
Wide QRS 3rd-degree block should not be treated with atropine but initially with TCP or beta-adrenergic medications IV. These treatments should be used temporarily until transvenous pacing is initiated. TCP should be provided immediately if the patient is unstable, without IV access, or medications prove ineffective.
If TCP cannot be used or is ineffective, the patient should be treated with:
- IV dopamine 5–20 mcg/kg/minute
OR
- IV epinephrine 2–10 mcg/minute
During this time, the clinician should:
- Obtain cardiac consultation
- Begin preparing for transvenous pacing