ECG Findings in Pulmonary Embolism
The utility of ECG for the diagnosis of pulmonary embolism is limited. However, it may be useful in detecting right ventricular overload, which is an important finding that can change patient management.
In acute and subacute pulmonary embolism, there is an increase in pulmonary artery resistance. The sudden rise in pulmonary artery resistance leads to a modest dilatation of the right ventricle and right atrium. The dilatation is caused by right ventricular overload and does cause some ECG changes.
- A thrombus lodged inside the pulmonary artery increases pulmonary arterial pressure.
- Acute pulmonary hypertension causes sudden right atrial and right ventricular enlargement.
Alterations of the QRS Complex
- Right-shifted ÅQRSF: SI/QIII (SI ≥ 1.5 mm; QIII ≥ 1.5 mm) or SI/rSr’III
- QRS clockwise rotation with a delayed transition zone or displacement leftward toward V5 and V6 caused by rotation of the heart in its horizontal axis
- Right ventricular conduction disturbance
-
- Incomplete right bundle branch block (iRBBB) with an rSr’ complex in lead V1
- RBBB with an rsR’ complex in lead V1
-
- A QR complex (Qr) in lead V1 if there is a massive pulmonary embolism causing obstruction of more than 80% of the pulmonary arteries
Changes in Repolarization
- Negative T waves in limb leads III and aVF
- Negative T waves in precordial leads V2 and V3, without iRBBB or RBBB
- ST depression in leads V1 to V3
- ST elevation in leads V1 and III
- ST or T alterations in the left precordial leads (V5/V6)
Disturbances in the Rhythm
Patients with pulmonary embolism will likely have the following rhythm abnormalities:
- Sinus tachycardia is present in 70–90% of patients.
- Atrial flutter is present in 5–10% of patients.
- Atrial fibrillation is a rare occurrence.
P Wave Changes
- The classical P pulmonale sign can be found with pulmonary embolism.
- P wave amplitude of about ≥ 2.5 mm in lead II
- P wave negative in aVL
- High peaked P waves in lead II and V2 are seen in P pulmonale vasculare.
Unreliability of ECG Findings with Pulmonary Embolism
The ECG diagnosis of acute pulmonary embolism is unreliable. Studies have shown that an ECG may not show signs of a PE despite patients presenting with overwhelming signs and symptoms of life-threatening acute pulmonary embolism such as:
- Severe dyspnea
- Tachypnea
- Hemoptysis
- Preshock symptoms
- Distended jugular veins
- Cyanosis
- Sinus tachycardia
The ECG diagnosis of PE has poor specificity and sensitivity. Many patients with preexisting ECG alterations may be misdiagnosed as having acute pulmonary embolism. Conversely, the ECG tracing may not show signs of right ventricular overload in the setting of acute pulmonary embolism.
It is often hard to distinguish a normal variant from right ventricular overload.
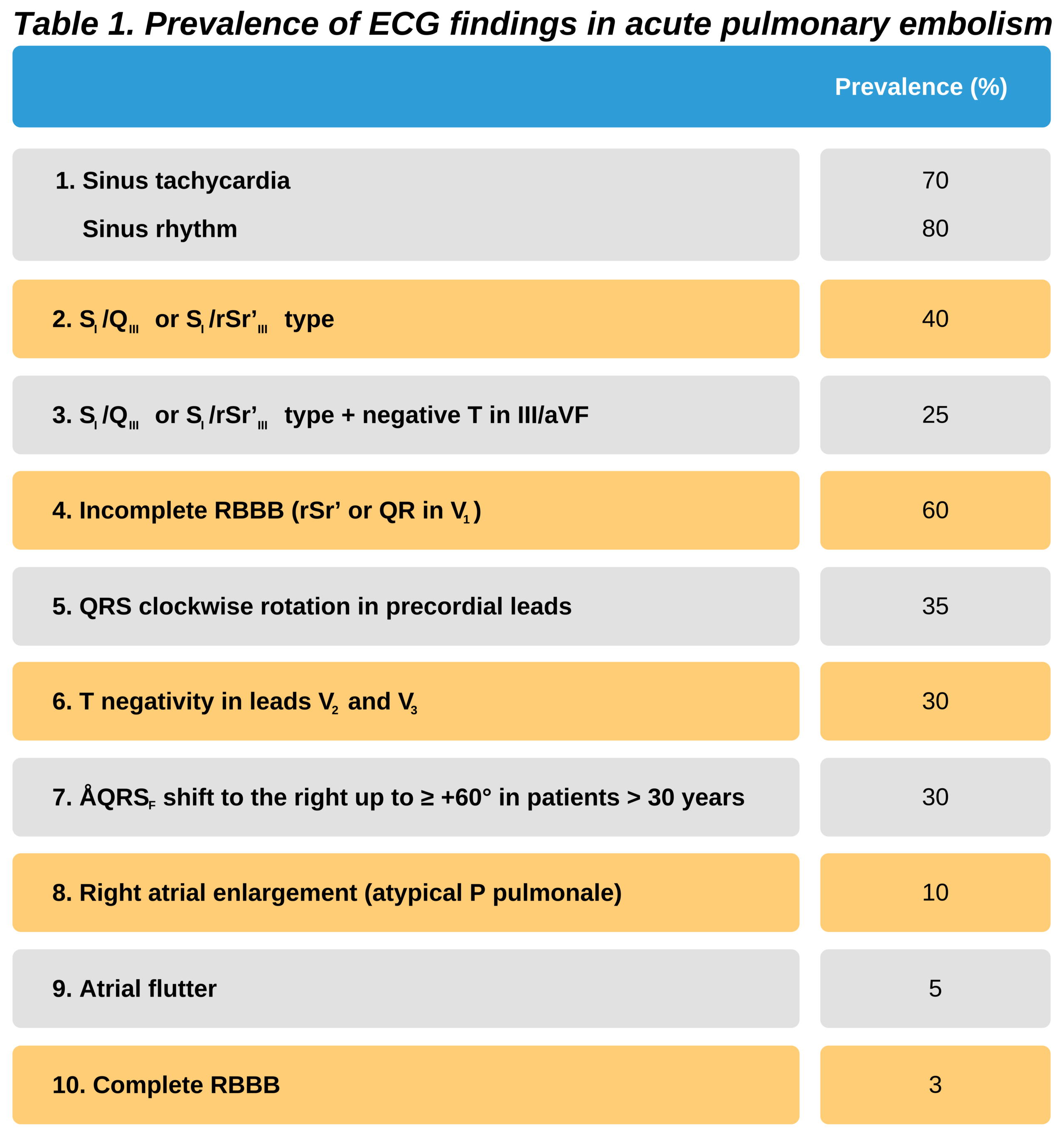
Table 1 presents the prevalence of the ECG findings associated with acute pulmonary embolism in patients diagnosed with a PE.