Atrial Flutter
Atrial flutter is more common in the older population. It can last for several beats or several years. Patients may be asymptomatic or hemodynamically unstable. Symptoms are dependent on the ventricular rate that the atrial flutter produces.
During atrial flutter, the atrial rate is 230–330 bpm and consistent. The atrial impulse is consistently blocked by the AV node in a ratio of 2:1. Consequently, the ventricular rate is kept at 130–150 bpm.
A RBBB may be present that masks the flutter waves and causes the ECG tracing to look like ventricular tachycardia. Atrial flutter with RBBB displays a tachycardia pattern with small or broad QRS complexes. It has a rate of 130–160 bpm. These findings are consistent in about 70% of patients.
The rate in atrial flutter can be pharmacologically slowed down to under 200 bpm by amiodarone. Physiologically, the atrial rate can be slowed down by a dilated right atrium due to excessive intra-atrial conduction disturbance.

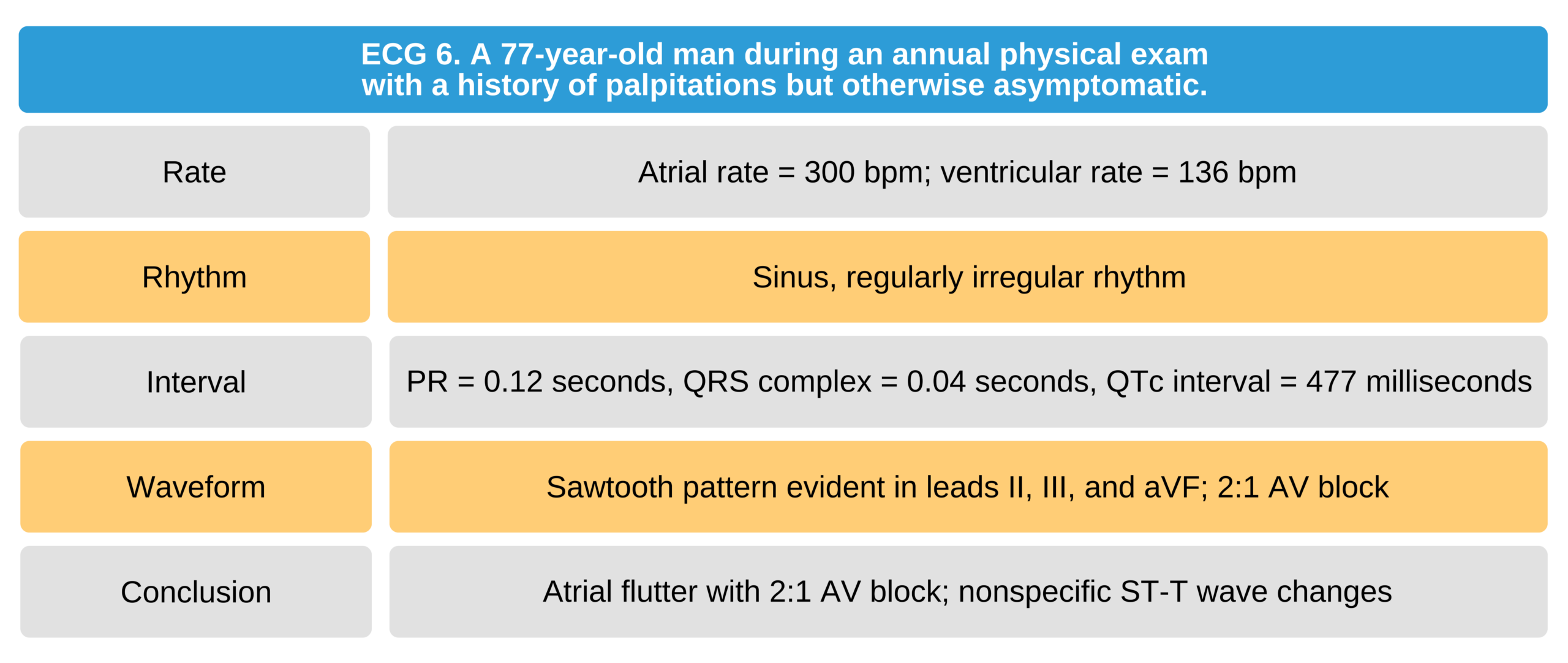
77-Year-Old Man With a History of Palpitations butOtherwise Asymptomatic ECG
Related Video – ECG Rhythm Review – Atrial Flutter
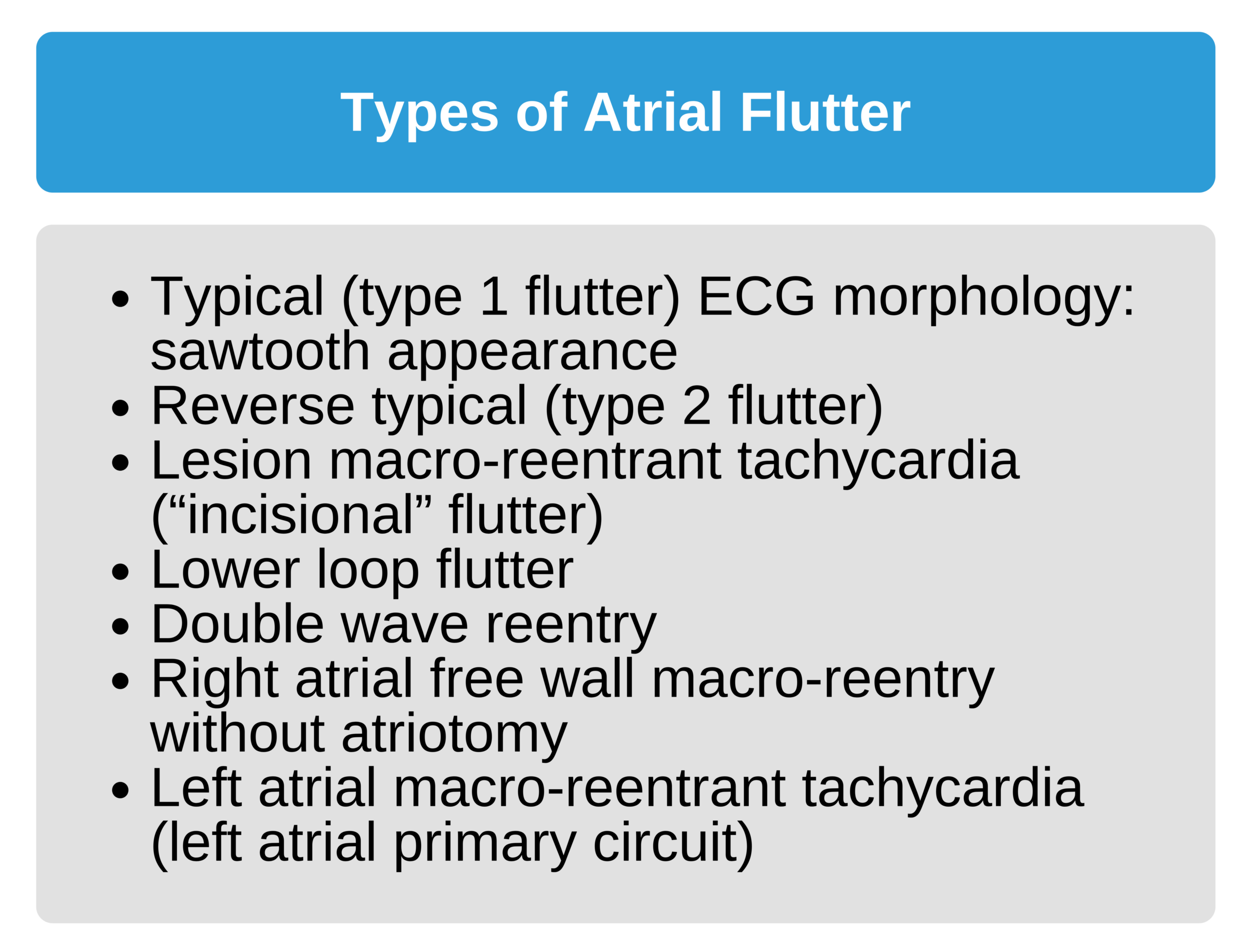
The Types of Atrial Flutter
Atrial flutter (AFL) is caused by a circuit that produces a macro-reentry of impulses inside the right atrium.
There are two types of atrial flutter:
- Type 1 atrial flutter follows a circuit that travels counterclockwise.
- Type 2 atrial flutter follows a circuit that travels clockwise.

Type 1 Atrial Flutter
Type 1 Atrial Flutter
Type 1 atrial flutter is the most common and is observed in 85% of patients diagnosed with AFL. Type 1 AFL generates a “saw-tooth” appearance on ECG in limb leads II, III, and aVF. The flutter or P-like waves are also visible in precordial lead V1. The isoelectric line can no longer be delineated.

Atrial Flutter “Saw-Tooth” Display on ECG
The second-degree AV block ratio varies from 2:1 to 4:1 or even higher. The ventricular rate fluctuates as the ratio of the AV block changes. A Wenckebach phenomenon may be superimposed on the ECG tracing of type 1 atrial flutter. Consequently, this can be mistaken for atrial fibrillation at first glance. With experience, one can distinguish the changes of AV conduction when studying a longer ECG strip.
An AV-block ratio of 1:1 occurs in children and in adults when the sympathetic nervous system is stimulated, e.g., during exercise. Patients with a preexcitation pattern such as Wolff-Parkinson-White syndrome may also have a 1:1 AV block. Likewise, patients taking quinidine for autoimmune disease and the treatment of malaria have been observed to exhibit a conduction rate of 1:1.
When atrial flutter reaches a ventricular rate of 300 bpm, the patient may progress to ventricular fibrillation.
Type 2 Atrial Flutter
Type 2 atrial flutter is uncommon and only seen in 15% of patients diagnosed with AFL. This type of atrial flutter lacks the saw-tooth appearance, and the isoelectric line is preserved. The flutter waves retain a recognizable P wave shape, and the P waves have a positive deflection in leads III and aVF.
The atrial rate ranges between 240 bpm and 280 bpm. The AV conduction is like type 1.
The P wave morphology in type 2 atrial flutter resembles that of atrial tachycardia because of the P wave-like flutter waves. Digitalis treatment is contraindicated in patients with atrial tachycardia and incomplete AV block.
Differentiating atrial flutter from atrial tachycardia is very difficult. Cardiac rate is one clue that can be used to differentiate them. Atrial tachycardia rarely exceeds 210 bpm.

Uncommon Atrial Flutter ECG 34
In the ECG above (figure 4), there are no sawtooth waves appreciated in leads III and aVF. P waves are visible. However, limb lead II does have a sawtooth appearance typical of AFL. This represents a clockwise reentry circuit, an uncommon variant.
34 Burns E. Atrial flutter. Life in the fastlane website. Accessed September 4, 2020.
https://litfl.com/wp-content/uploads/2018/08/ECG-Atrial-Flutter-variable-block-2-1-4-1.jpg