Electrocardiographic Findings
There are three ECG findings to watch for when evaluating a patient’s ECG for RVH:
- Absence of right ventricular conduction disturbance
- The presence of an incomplete RBBB
- The presence of complete RBBB
An ÅQRSF of > +90° is often present. ST depression and T wave inversion in leads V1 through V2 or V3 is present in category 1 and 2 RVH.

Right Ventricular Hypertrophy Video
Right Ventricular Hypertrophy without Right Ventricular Conduction Disturbance
Three characteristics in lead V1 of an ECG suggestive of RVH:
- Pure R wave in a positive QRS deflection
- 1:1 R/S ratio in lead V
- R wave > 7 mm, S wave < 2 mm
A single positive deflection of the QRS complex in lead V1, depicting a pure R (see Figure 1), is the distinguishing ECG finding when RVH is present. This is usually seen in patients with severe pulmonary valve stenosis and in severe RVH associated with congenital heart diseases such as Eisenmenger syndrome. In patients with mitral stenosis and severe cor pulmonale, the R is often smaller in amplitude compared to the other two disease conditions.
These patients also present with an ÅQRSF of > +120°.

ECG Tracing of a 22-Year-Old Man With a Large VSD
The significant R complex in V1 is specific for RVH if there is no posterior MI and one type of preexcitation.
The presence of a qR complex in lead V1 is indicative of right ventricular overload. The Q wave in this instance corresponds to RVH and dilatation of the right atrium and right ventricle. This is not a significant finding of an old anteroseptal necrosis or infarct.

12-Lead ECG of a 46-Year-Old Woman With Severe Mitral Stenosis and Tricuspid Regurgitation
An R/S ratio of 1:1 or greater in lead V1 , is indicative of RVH. An R wave of > 7 mm or an S wave of < 2 mm in V1 are also findings in RVH.

ECG Tracing of Patient With RVH Secondary to Arrhythmogenic Right Ventricular Cardiomyopathy
Right Ventricular Hypertrophy with Incomplete RBBB and a Normal QRS Duration
The RSR Complex
- rSr’ complex in V1, where r’< r = normal variant
- rSr’-complex, where r’> r + negative T waves in V1 through V3 = RVH
Healthy, young patients may have an rSr’ complex in lead V1 as a normal variant. When the r’ wave is smaller than the initial R wave, this finding is rarely associated with RVH.
About 40% of patients with an r’ wave larger than the initial R wave do have RVH. Negative T waves in V1 through V3 further support a diagnosis of RVH.
The rSr’ type where the r’ > r wave is usually seen in patients with:
- Atrial septal defect who also have asymmetric negative T waves in V1 through V3
- Chronic pulmonary embolism
- Valvular pulmonary stenosis
- Mitral stenosis
This pattern can also represent an intermediate state between incomplete and complete RBBB.
Note: Patients with barrel chests can also present with an rSr’ type where the r’ > r wave. This is often considered a normal variant.

12-Lead ECG of a 52-Year-Old Woman With an Atrial Septal Defect
RVH with Complete RBBB and Prolonged QRS
When differentiating RBBB from RVH, the clinician should keep in mind that there is a typical pattern of an rsR’ complex in lead V1 that suggests the presence of RBBB with or without RVH. Additionally, sometimes only a single notched R wave is present without an S wave. Of note, the T wave is always negative in leads V1 through V4 with or without RVH.
Right ventricular hypertrophy appearing with RBBB can only be diagnosed if:
- The amplitude of the R’ wave > 12 mm
- The QRS duration is > 0.14 seconds due to the notching in the R wave
- The ÅQRSF is +80° to +120°
Patients with cor pulmonale usually have a P pulmonale finding on the ECG as well, representing the cardiac effects of their chronic pulmonary hypertension.
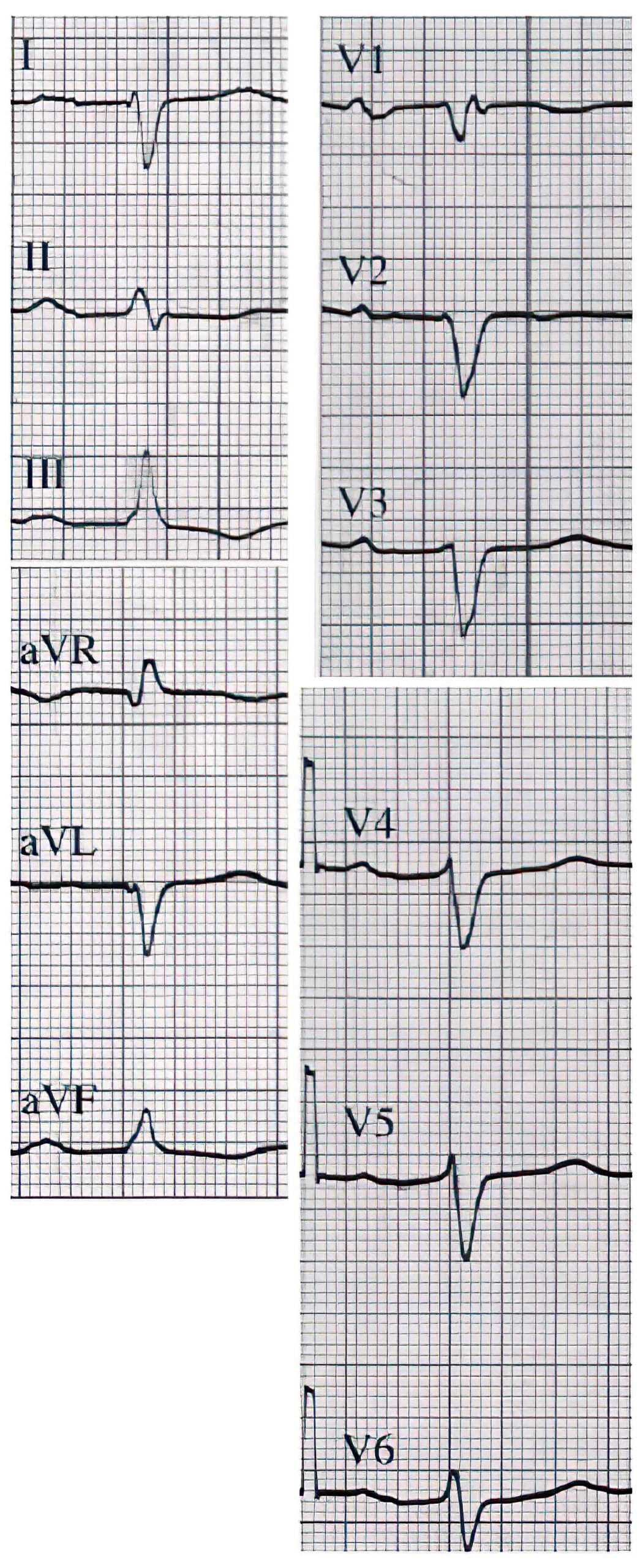
Figure 5. 12-lead ECG of a 68-year-old man with COPD, global respiratory failure, and right ventricular failure. ÅQRSF is +110°, and an rS complex is present in all precordial leads.
Perils and Pitfalls
RBBB is found more frequently in patients without RVH. Therefore, echocardiography is recommended to confirm the presence of RVH in these cases.
Rare RVH Patterns
Some variations in ECG patterns that may indicate RVH include an SI/SII/SIII pattern.
RVH can also be seen as a negative QRS complex in all precordial leads with or without incomplete RBBB and with the frontal plane QRS complex showing right axis deviation.