Other Causes of Q Waves
Myocardial infarction is not the only cause of a Q wave:
- Q wave in limb lead III is a normal variant
- Septal hypertrophy
- Hypertrophic obstructive cardiomyopathy
- Situs inversus
- Conditions such as amyloidosis and cardiomyopathy that cause myocardial scarring, which impairs impulse conduction
- Poor lead placement
When a Q wave cannot be attributed to any known disease, the diagnosis of unclear etiology is made.

An ECG of a patient without cardiac problems, and one of a patient with inferior wall MI and lateral wall ischemia.
False Lead PolingWhen the upper limb leads aVR and aVL are interchanged, limb lead I presents a mirror image pattern of the normal lead I.

One ECG (a) with correct limb lead placement and one (b) where they are interchanged. 22
As shown in the ECG above, when leads aVR and aVL are interchanged, lead I becomes a mirror image of the normal lead I morphology. Limb leads II and III as well as leads aVL and aVR switch places. Limb lead aVF remains unchanged.
A guide to detecting aVL and aVR reversal:
- Lead I is completely inverted, including the P wave, QRS complex, and T wave.
- Lead aVR becomes positive.
- Right axis deviation may be noted.
Anytime an ECG interpretation suggests a rare disease such as situs inversus or an anterior wall MI, the clinician should check for possible false poling.
Left Ventricular Hypertrophy
LVH may produce a Q or QS wave in limb leads III or aVF. The ECG of a patient with severe aortic valve incompetence may develop a deep Q wave of 0.025 seconds and up to 2.5 mm in leads V5 and V6.
Left Bundle-Branch Block
A QS wave in limb lead III with positive asymmetric T waves is seen in LBBB. LBBB sometimes manifests QS waves and minimal r waves in precordial leads V1 through V4. The QRS duration in LBBB is longer than 0.14 seconds.
Wolff-Parkinson-White Syndrome
Posteroseptal preexcitation in Wolff-Parkinson-White syndrome produces delta waves and a negative QRS complex in limb leads III and aVF.
Hypertrophic Obstructive Cardiomyopathy
There are many patterns in hypertrophic obstructive cardiomyopathy that may produce Q waves:
- There may be q waves in leads V5 and V6.
- The Q waves may be as long as 0.04 seconds.
- On rare occasions, negative QRS complexes may appear in all leads except aVR.
The ECG of patients with hypertrophic obstructive cardiomyopathy may not exhibit Q waves at all and instead show signs of LVH, LBBB, or even normal ECG patterns despite the presence of significant intraventricular systolic function.

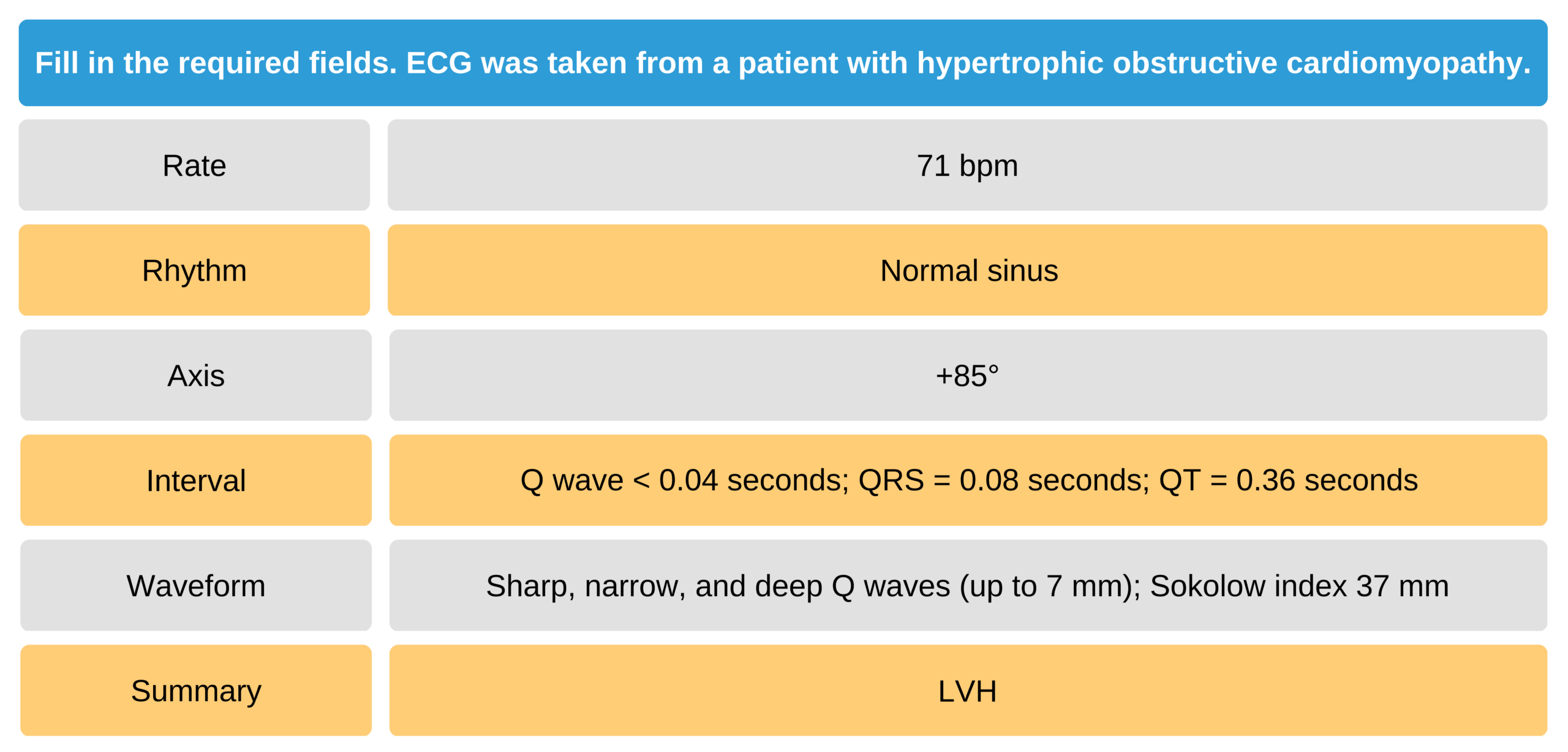
Hypertrophic Cardiomyopathy ECG Rhythms 23
This ECG tracing came from a patient with hypertrophic cardiomyopathy. There is left ventricular hypertrophy with a positive Sokolow index of 37 mm (12 mm [SV1] + 25 mm [RV6]). Deep and narrow Q waves are visible in the inferolateral leads (I, II, III, aVF, V5, and V6). A narrow Q wave of < 0.04 seconds lets the clinician rule out MI.
Situs Inversus
Patients with situs inversus have ECG changes similar to false poling that occurs when leads aVL and aVR are interchanged. Situs inversus also presents with abnormalities in the precordial leads V1 through V6. The ECG tracing in the precordial leads shows decreased R waves and increased S waves, especially in leads V2 through V6.
When the ECG leads are placed on the right thoracic area, the tracing reads normally. This change in lead placement confirms the diagnosis of situs inversus.
Surgically Corrected Transposition of the Great Arteries
Transposition of the great arteries is a congenital heart anomaly where the ventricles are interchanged. Consequently, ventricular septal depolarization produces vectors that move from right to left. The ECG shows small q waves and a qrS complex in leads V1 and V2; leads V5 and V6 do not have q waves.
Other Conditions for Pathologic Q Waves
Pathologic Q waves have been reported in patients after pneumonectomy and pericardiectomy and in patients with pneumothorax. Patients with Duchenne muscular dystrophy who have developed hypertrophic cardiomyopathy and patients with cardiac amyloidosis may also have pathologic Q wave findings.
QR or Qr complexes in lead V1 have been reported in patients with massive acute pulmonary embolism or severe mitral stenosis with tricuspid incompetence. This finding is conclusive for severe right atrial dilatation.
22 Burns E, Buttner RB. ECG limb lead reversal. Life in the fastlane website. Accessed August 3, 2020.
https://litfl.com/wp-content/uploads/2018/08/ECG-Leads-LA-RA-Reversal.jpg
23 Burns E. Hypertrophic cardiomyopathy. Life in the fastlane website. Accessed August 1, 2020.
https://litfl.com/wp-content/uploads/2018/08/ECG-HCM-Dagger-Q-waves–1024×356.jpg