Chapter Progress
0% Complete
Get 12-Lead ECG Certified Today
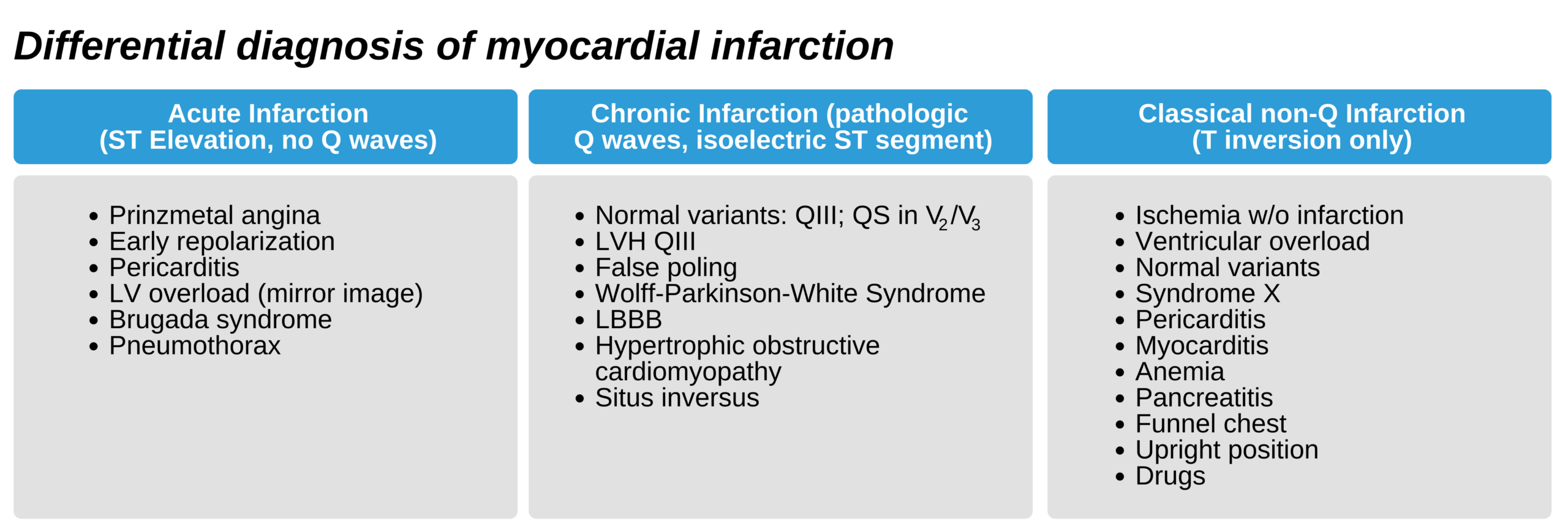
Differential Diagnosis of Myocardial Infarction ECG Patterns
ECG findings suggestive of MI overlap with other clinical conditions. When evaluating a patient, the clinician must consider MI along with other diagnoses as part of the differential.
ECG is an important tool in the diagnosis of MI. However, the clinical history and physical diagnosis, together with laboratory findings, such as serum troponins, creatine kinase, and CK-MB, are equally as important.
- Patients with pericarditis have ST elevation changes of < 3 mm that do not develop into pathologic Q waves. The ST elevation is a mirror image of ST depression caused by left ventricular overload or LBBB. It is also seen in early repolarization changes and Brugada syndrome.
- ST elevations in leads V2 and V3 with insignificant amplitudes may be a normal variant.
- ST elevations that return to the isoelectric line within 20 minutes, with or without chest pain, may be due to Prinzmetal angina. Patients with this condition may need to undergo coronary angiography to rule out significant occlusions.
- Ischemia without necrosis, subacute and chronic pericarditis, and cardiac syndrome X may cause symmetrical T waves of 2–7 mm in amplitude in multiple precordial leads and in limb leads I, II, and/or aVL.
- Patients with hyperkalemia and sinus bradycardia may have tall, positive, and symmetrical T waves in precordial leads V2 and V3.