Third-Degree AV Block, Complete AV Block
In third-degree AV block, impulse conduction between the atria and ventricles is completely blocked. The atria follow an atrial rhythm, while the ventricles independently follow a ventricular escape rhythm, e.g., an AV nodal rhythm.
If the ventricle fails to respond with an escape rhythm, then ventricular asystole occurs. The extent of the patient’s clinical symptoms depends on the duration of ventricular asystole.
- Dizziness and presyncope are common if asystole lasts for 3–6 seconds.
- Syncope is likely if asystole lasts > 6 seconds.
Patients with other medical conditions may experience syncope after ventricular asystole of only 3 seconds. If asystole lasts 4–7 minutes, irreversible end-organ damage is likely, especially in the brain. Longer ventricular asystole may lead to death. A Stokes-Adams attack is a syncopal event caused by a cardiac arrhythmia.
Infra-His third-degree AV block has lesions below the bundle of His, and in supra-His third-degree AV block, the lesions are located above the bundle of His.
Related Video -ECG Rhythm Review – 3rd Degree (Complete) Heart Block

The Bundle of His, the supra-His, and the infra-His
Infra-His Third-Degree AV Block
Infra-His third-degree AV blocks are localized distal to the bundle of His. Their origin can be found within the ventricular fascicles and bundles. Coronary artery disease and idiopathic fibrosis of the infra-His conduction system (Lenègre disease) are the usual causes. Fascicular blocks, bundle-branch blocks, and bilateral bifascicular blocks are precursors of infra-His third-degree AV blocks.
The ventricular escape rhythm of the infra-His type averages 40 bpm but may be between 10 bpm and 45 bpm. The rate does not increase during strenuous activity. Episodes of asystole are also more frequent. Consequently, the patient’s hemodynamics are severely compromised.
Supra-His Complete AV Block
A supra-His third-degree AV block is localized proximal to the bundle of His in the region of the AV node. First-degree AV block and second-degree AV block Mobitz type I and advanced types are precursors to a supra-His complete AV block. A complete supra-His AV block can be caused by an acute inferior wall MI or digitalis toxicity. Rarer causes of the supra-His third-degree AV block include infectious and congenital heart disease.
Supra-His complete AV blocks are reversible in 90% of cases. A temporary pacemaker may be necessary to treat the patient. In the case of digitalis toxicity, clearance of the drug reverses the effects.
The AV junctional escape rhythm in the supra-His AV block generates a ventricular rate of 45–65 bpm. The escape rhythm is often stable and may last for months or even years.
The hemodynamics of patients with a supra-His AV block are usually less impaired than those of patients with an infra-His third-degree AV block. Episodes of asystole are rare. When the patient exercises, the ventricular rate can increase to 100 bpm.
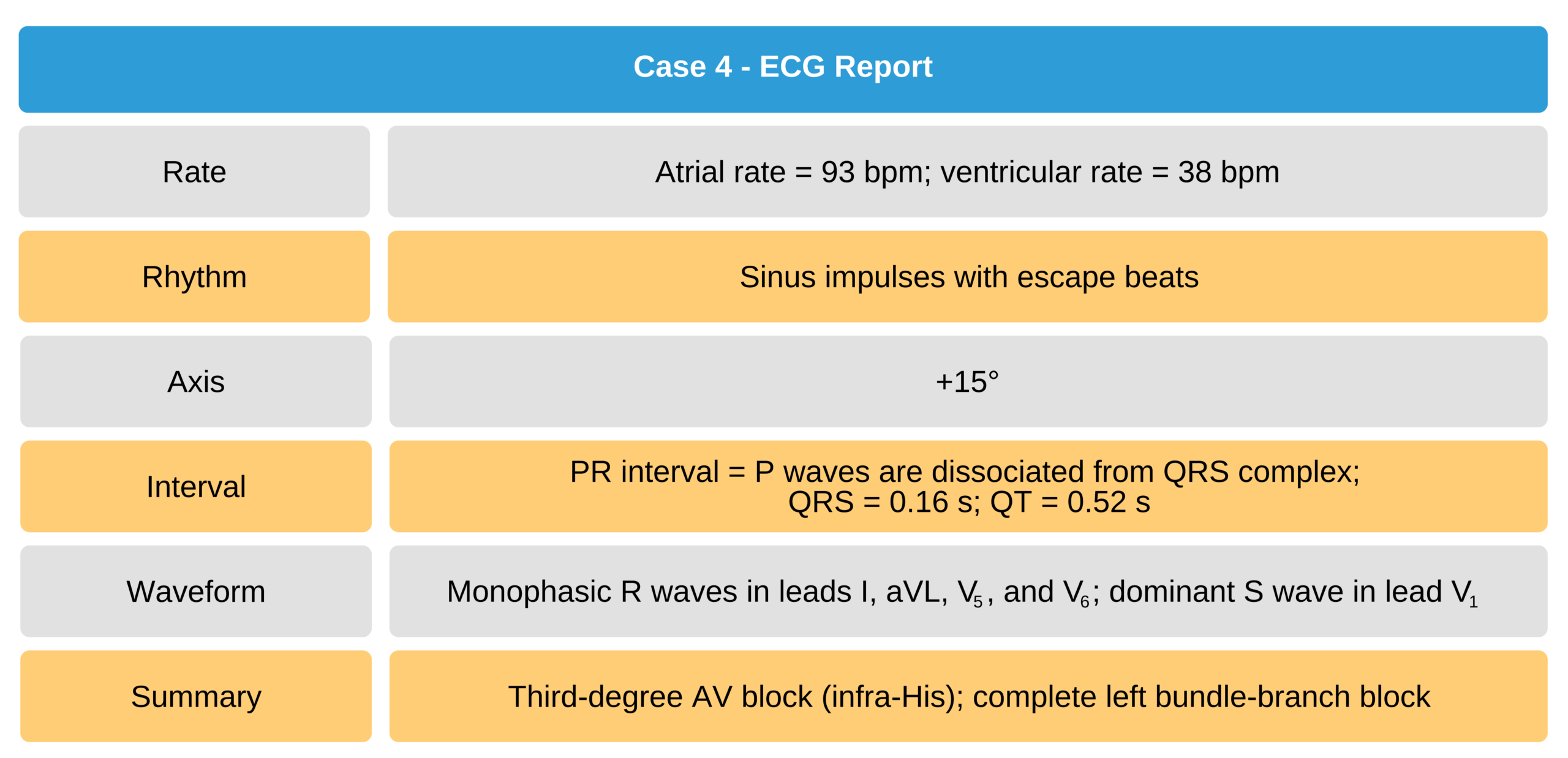
Case 4
72-year-old man with presyncopal symptoms.

72-Year-Old Man With Presyncopal Symptoms ECG

72-Year-Old Man With Presyncopal Symptoms ECG Isolated Lead V1