Complex Infarction Patterns
Complex infarction patterns occur when the MI coexists with a classical intraventricular conduction defect such as LBBB, RBBB, left anterior fascicular block (LAFB), left posterior fascicular block (LPFB), and bilateral fascicular blocks.
Chronic Myocardial Infarction + LBBB
Chronic MI associated with LBBB has the following ECG findings:
- A q wave in at least two of these leads: I, aVL, V5, and V6
- Regressing r wave amplitude across V1 through V4
- Notching of the S wave in V3 through V5 — known as the Cabrera sign
Acute MI with LBBB may manifest with ST elevations instead of the usual ST depressions.
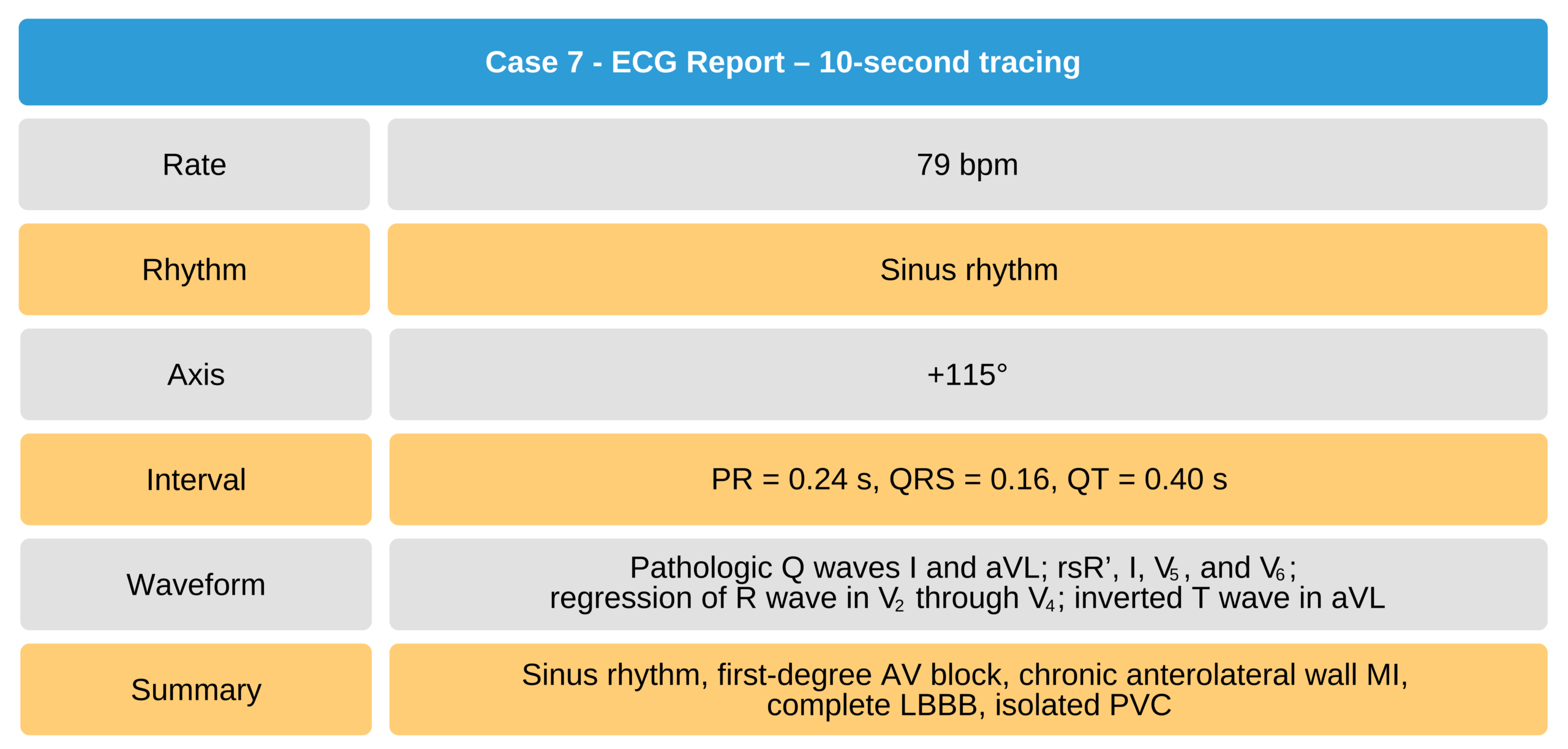
Case 7
A 56-year-old woman with 2-year history of two-vessel coronary artery disease, s/p PTCA.

56-Year-Old Woman With Two-Vessel Coronary Artery Disease ECG
Chronic Myocardial Infarction + RBBB
Chronic MI associated with RBBB manifests in the inferior and anterior regions, making it easier to identify. Pathologic Q waves signifying necrosis occur at 0.4 seconds of the QRS complex even if the patient has RBBB. The RBBB manifestations occur in the last 0.5 to 0.6 seconds of the QRS complex.
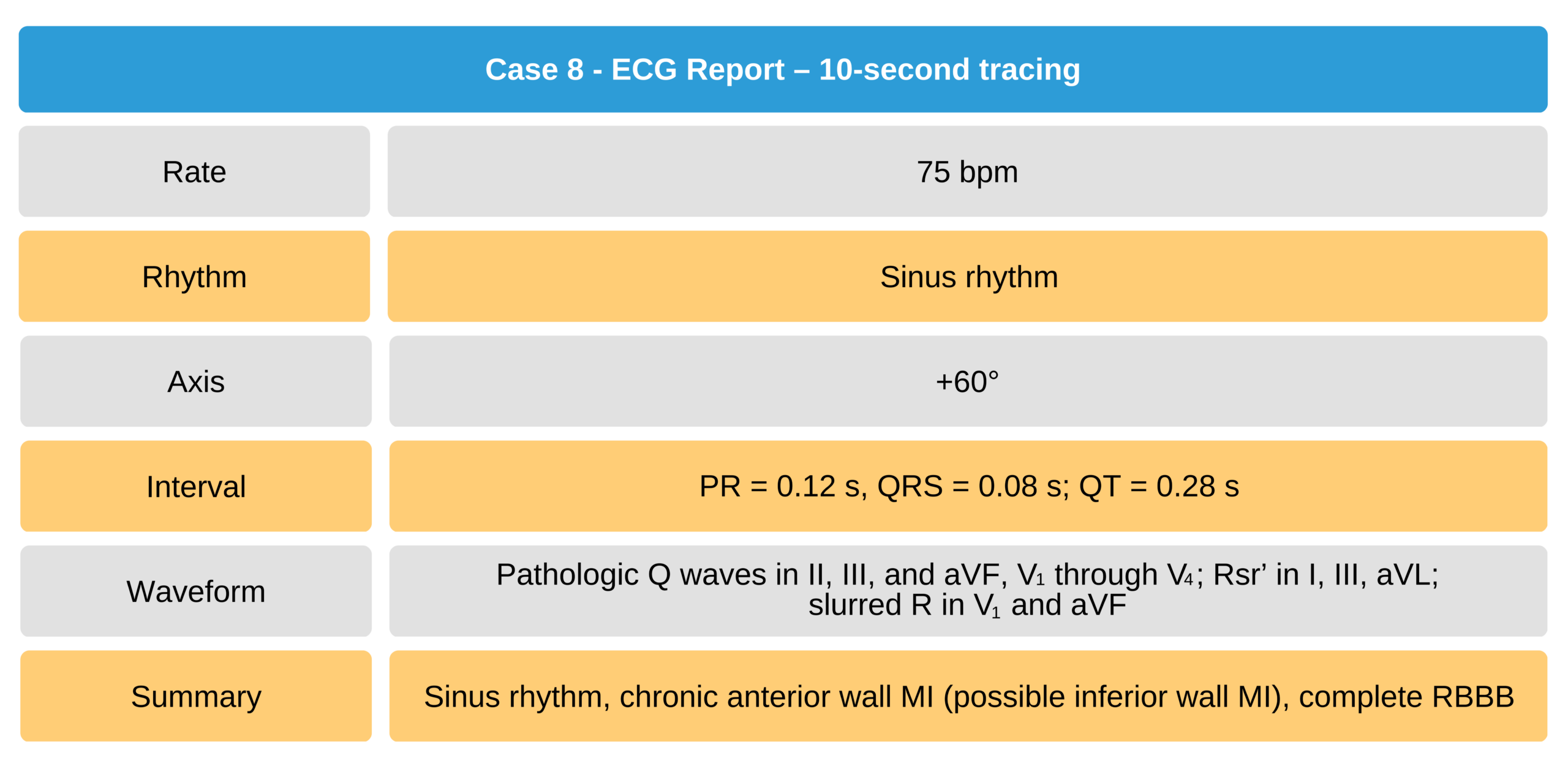
Case 8
A 63-year-old man with an old anterior wall MI, a possible old inferior wall MI, and RBBB.

63-Year-Old Man With Old Anterior Wall MI and RBBB ECG
Myocardial Infarction with Left Fascicular Block
Left anterior fascicular block usually masks an anteroseptal wall MI. In some cases, it may also mask an inferior wall MI. However, an extensive anterior wall MI is detectable on ECG despite the presence of LAFB. Case 9 is an example of a 39-year-old man with chronic inferior wall MI and LAFB.
Left posterior fascicular block is a rare conduction disturbance only seen in a small number of patients with an inferior wall MI. LPFB completely masks inferior wall MI findings.
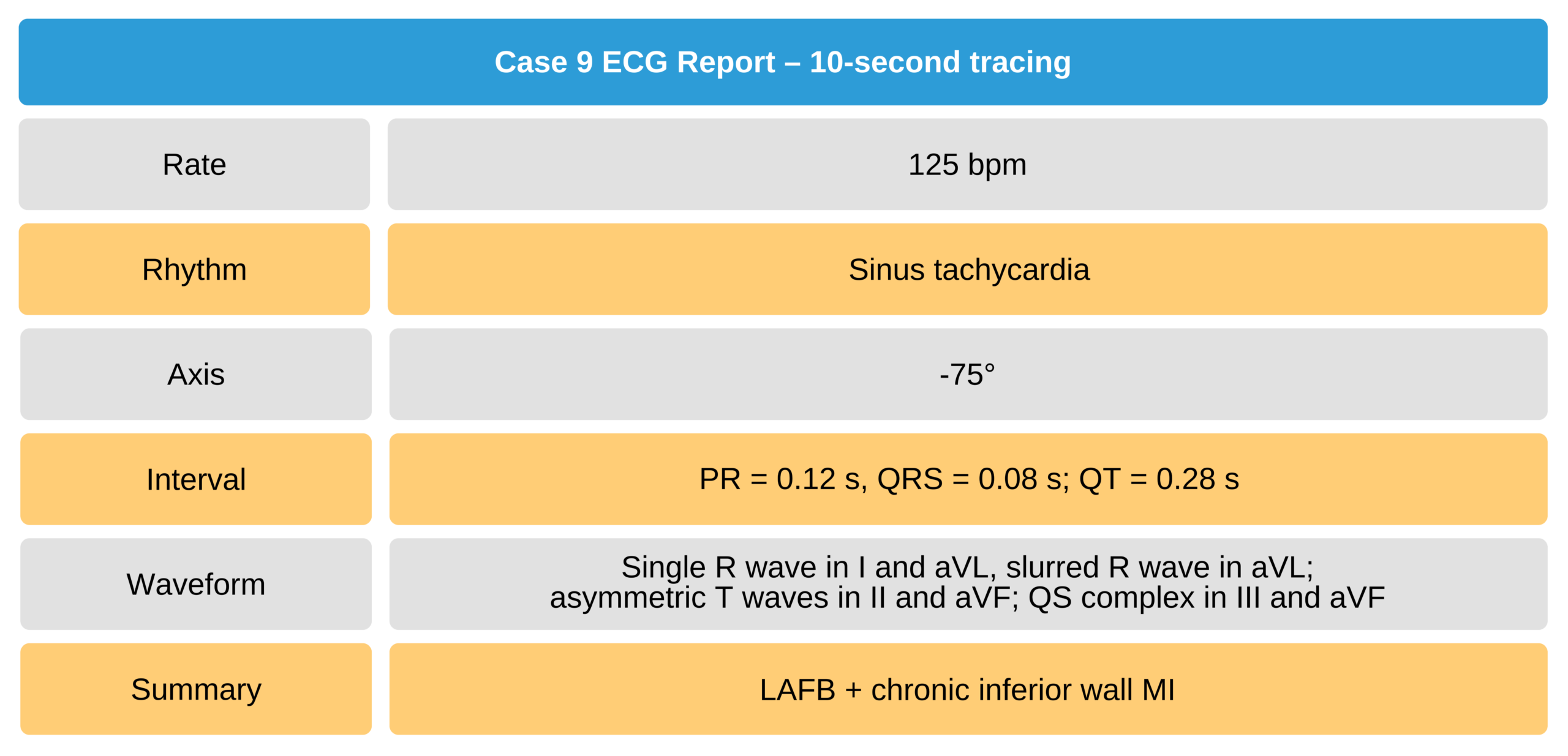
Case 9
A 39-year-old man with an inferior wall MI and LAFB.

39-Year-Old Man With Inferior Wall MI and LAFB ECG