Medications
Medications to treat VF, such as vasopressors or antiarrhythmics, should only be given if primary treatments, CPR, and defibrillation, are ineffective. The Cardiac Arrest algorithm for adults states that these medicines should be given only if VF is persistent after CPR and defibrillation. Patients who have refractory VF should receive medications earlier as their benefit is greatest when given early. The administration of medications should never delay CPR or defibrillation.
Vasopressive Medications
Vasopressive medications increase diastolic blood pressure, thereby increasing CPP (coronary perfusion pressure). CPP determines successful ROSC, while cerebral perfusion pressure determines the return of brain function.
Key Takeaway
The most important determinant of successful resuscitation is effective CPR and defibrillation when a shockable rhythm is present.
Cardiac output (CO) is determined by heart rate and stroke volume (CO = HR x SV). Poor cardiac output and decreased oxygen delivered to tissues are common in cardiac arrest. During this early state, the body compensates by increasing the systemic vascular resistance (SVR). Therefore, a detectable blood pressure (BP = CO x SVR) does not necessarily indicate adequate cardiac output. Additionally, even if cardiac output is maintained, tissue perfusion may not be maintained if there is poor oxygen uptake or delivery. For example, a low concentration of hemoglobin or arterial oxygen pressure may also decrease tissue perfusion.
Epinephrine is a vasopressive medication due to its alpha-adrenergic effects and is a useful adjunct during cardiac arrest. The alpha-adrenergic effects lead to an increase in CPP and cerebral perfusion. However, it is important to note that epinephrine also has some beta-adrenergic effects, which theoretically may increase the work of the heart and decrease perfusion to the inner layers of the heart.
Physiologic Mechanism of Vasopressive Medications
Receptor Mechanism
Receptors are the molecules on cells that interact with chemical agonists, which can be hormones or neurotransmitters. The chemical agonist stimulates the receptor leading to a cascade of events that causes changes within the cell and results in a biologic effect.
Autonomic or sympathetic agonists act on the involuntary nervous system, including the cardiovascular system. Examples include epinephrine (from the adrenal glands) and norepinephrine (from some nerve terminals). Following activation of the receptor, a secondary effect is increased calcium within the cell. In myocytes (muscle cells), the increase in calcium leads to contractions of the cells. This pathway is called signal transduction.

Signal Transduction Pathway
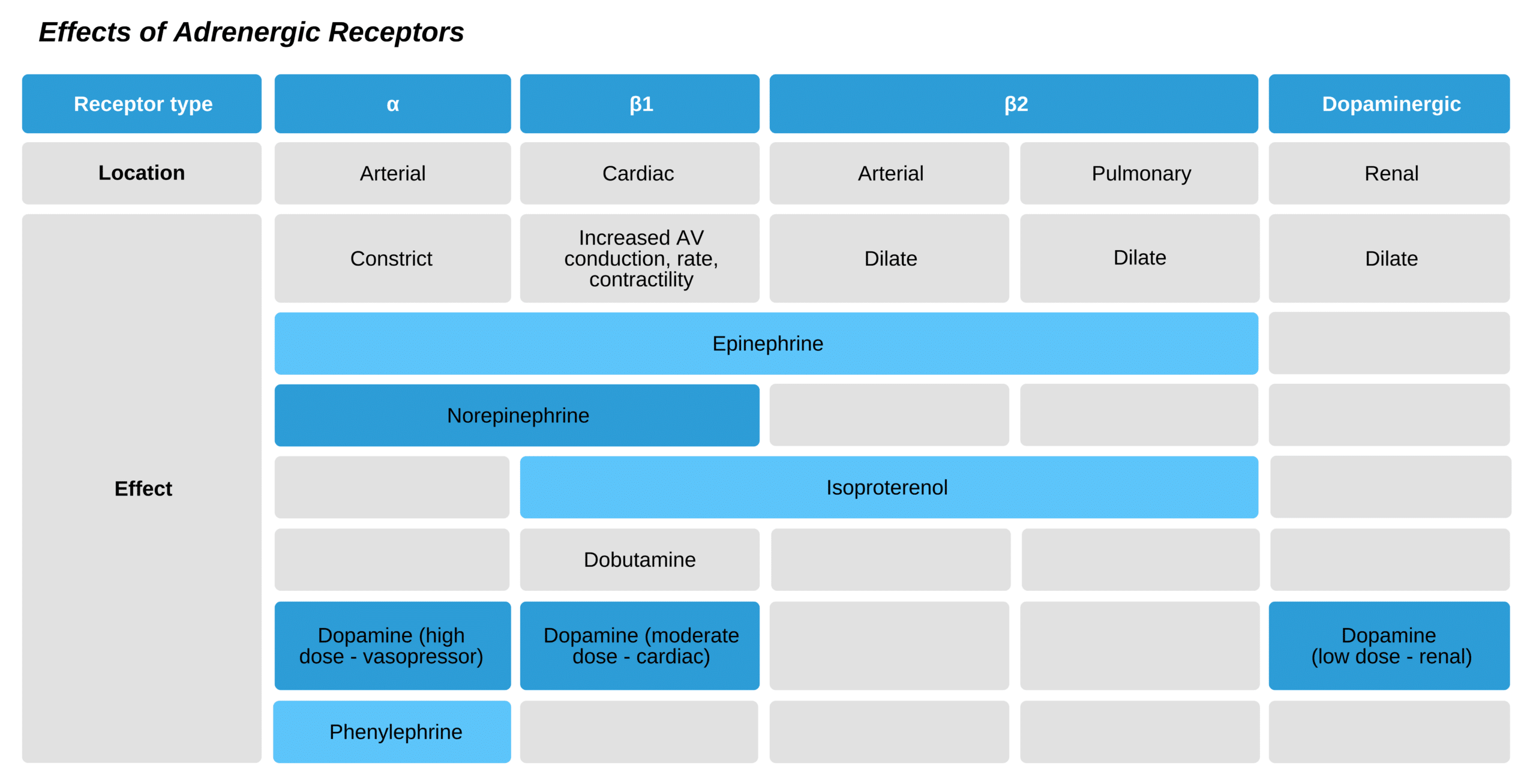
Adrenergic Receptors
These receptors affect the autonomic (involuntary) nervous system, including vascular, cardiac, pulmonary, and intestinal smooth muscle. There are three major sub-categories:
- Alpha (α 1, α 2)
- Beta (β1, β2)
- Dopaminergic
The alpha receptors affect the smooth muscles of the vasculature and have an effect during cardiac arrest and the post-cardiac arrest period. Stimulation ultimately leads to vasoconstriction, resulting in an increase in blood pressure. There is a range of effect of the various alpha-adrenergic agonists (also called catecholamines):
Norepinephrine>Epinephrine>Dopamine>Phenylephrine
Alpha receptors are found in cardiac muscle cells and lead to increased contractility (inotropic effect). However, there is also a beta effect on the cardiac muscles, which increases the oxygen needs of the cardiac muscle cells, which is not beneficial during arrest. The beta effect on the cardiac muscles is more pronounced than the alpha effect.
The β1 and the β2 receptors are the most active of the beta-type receptors.
- β1 receptors have excitatory action and are abundant at the sinus node and cardiac ventricles. Their effect is inotropic (increased cardiac contractility) and chronotropic (increased heart rate).
- Β2 receptors are located all over the body and cause relaxation. Consequently, they lead to vasodilation as well as bronchodilation.
Dopaminergic receptors are found in the smooth muscle cells of the brain, heart, kidney, and abdominal vasculature. The main outcome of activating these receptors is dilation of the vasculature. Additionally, in the kidney, they inhibit sodium reabsorption in the proximal renal tubules, leading to overall sodium excretion. And in the pituitary gland, they stimulate thyroid and prolactin hormone release.
Pharmacologic Effects
The physiological effects of adrenergic medications differ from person to person. This is because pharmacokinetics (the interaction of medicine dose and concentration in the plasma) and pharmacodynamics (the interaction of the concentration in the plasma and clinical outcomes) have several determinants. These include the effect on the receptor, other agonists that also activate the receptors, and the downstream effects of stimulation that can differ among patients. Importantly, a specific medication can affect multiple receptors (α, β1, β2, and dopaminergic), causing varying effects. Receptors have different activities based on their sensitivity to the agonists.
Other factors that affect medication outcomes:
- The density of receptors: this refers to the amount of cell surface receptors.
- The function of receptors: this can be influenced by other types of receptors and body functions.
- The parasympathetic nervous system
- Vasoactive substances like prostacyclin, endothelium relaxing factor, and thromboxane A2
- Endothelial dysfunction: this can change the body’s responses to medications.
These interactions are quite complex and differ from patient to patient. They are also affected by the patient’s physiology. As a result, responders must be prepared to adjust the dose of medications, as one dose will not work the same way for all patients and in all situations. The medications and doses must be carefully evaluated as well as the patient’s response to these medications.
Cardiac Arrest and Epinephrine
Epinephrine causes both alpha and beta-adrenergic responses. However, the alpha effects are most important for their benefits in cardiac arrest. The most significant primary effect is an increase in cardiac and cerebral perfusion.
Despite its widespread use in managing VF and pVT, there is no consistent research showing that it improves survival in patients.
Key Takeaway
Negative effects of using epinephrine during cardiac arrest:
At low doses, it causes poor kidney function and reduced urine output.
It can cause increased risk of arrhythmias and hyperadrenergic states.
It increases the work of the cardiac muscles, leading to increased oxygen requirements.
IV dosing of epinephrine leads to:
- Increased vascular resistance
- Increased blood pressure
- Increased heart rate
- Increased force of the heart contraction
- Increased blood flow to the brain and heart
- Increased oxygen requirement for cardiac muscle cells
- Automaticity
Key Takeaway
When giving epinephrine, each bolus should be followed by a 20 mL saline flush, and the extremity should be raised above heart level for 10–20 seconds.
Epinephrine is useful in the following situations:
- Cardiac arrest (asystole and PEA, persistent VF and pVT)
- Bradycardia with symptoms (following atropine failure)
- Significant hypotension (due to shock, may be contraindicated in pts with significant cardiovascular disease)
- Anaphylaxis
The standard dose is 1 mg, although this dosing is based on non-human research and intracardiac dosing in humans. This dose is not based on patient weight. Generally, a standard dose of 1 mg given at 3- to 5-minute intervals is used in cardiac arrest. (Class IIb, Evidence level B-R).
Epinephrine should be given after the second shock in patients with shockable rhythms.
There is no conclusive evidence (i.e., randomized controlled studies) that higher doses or increasing doses are beneficial in the general cardiac arrest patient. There is also concern that high doses can be damaging by increasing cardiac muscle dysfunction and a state of toxicity caused by excessive adrenergic activity following resuscitation. Consequently, using epinephrine at higher doses for cardiac arrest is not recommended. (Class III- not beneficial, Evidence level B-R) The provider can administer higher doses for specific indications such as an overdose of beta-blockade or calcium channel blockade. High doses of epinephrine are no longer recommended for cardiac arrest.
Related Video: Epinephrine – ACLS Drugs
Administering Medications in VF
When providing medications for VF, chest compressions must be ongoing to allow medication delivery to the heart. During cardiac arrest, chest compressions maintain only a fraction of the normal cardiac output (between 15 and 20% when optimal).
When a shock is delivered, this can depolarize the heart for a brief moment, causing asystole. During this period, anti-arrhythmic medicines have the following beneficial effects:
- They inhibit fibrillatory cardiac muscle action potentials.
- They augment coordinated cardiac muscle action potentials.
Anti-arrhythmic drugs historically have not shown a survival benefit. For decades, lidocaine has been used for cardiac arrest due to anecdotal evidence. Due to the lack of objective evidence, lidocaine is considered “class indeterminate” by the 2000 International Guidelines Conference. This was supported by the ILCOR Conference in 2010.
Currently, anti-arrhythmic drugs demonstrate only short-term benefits (e.g., ROSC or survival to hospital admission) when used for cardiac arrest due to VF or pVT. But there is no good evidence that long-term outcomes are affected, although small improvements may be difficult to detect with research.
Due to these equivocal results, the priorities of resuscitation, CPR, and defibrillation always take precedence over anti-arrhythmic administration. Administering these medications takes personnel and time, and this should never delay compressions or defibrillation. On the other hand, if a team member is available, and it will not delay necessary care, they should be given as quickly as possible as early intervention is preferred because their efficacy diminishes over time.
Cardiac Arrest and Amiodarone
Anti-arrhythmic medications are used when VF persists following high-quality CPR, defibrillation, and epinephrine. One of the two first-line medications used in this situation is amiodarone. The dose is 300 mg given as an IV or IO bolus, followed by a second administration of 150 mg IV after 3–5 minutes. Research in nonarrest VT showed a 40% response rate, and amiodarone has fewer side effects (such as clinical hypotension) than other antiarrhythmics. A water-soluble option is available, which has diminished the secondary effects previously seen, bradycardia and hypotension.
Related Video: Amiodarone – ACLS Drugs
Cardiac Arrest and Lidocaine
Lidocaine is another option and is dosed at 1.0–1.5 mg/kg IV at first dose then 0.5–0.75 mg/kg every 5–10 minutes up to 3 mg/kg. (Class IIb, Evidence level C-LD).
Key Takeaway
When using lidocaine:
- Do not use as prophylaxis in acute MI.
- Decrease the dose in patients with liver or heart failure.
- Monitor for neurologic compromise and stop the infusion immediately.
Related Video: Lidocaine – ACLS Drugs
Magnesium
IV and IO magnesium is used to stop torsades de points, which manifests as an irregular and polymorphic VF waveform. (Class IIb, Evidence level C). Magnesium infusion is not routinely used in patients in cardiac arrest with other forms of VF (Class III- not beneficial, Evidence level B-R) unless there is torsades or suspicion for hypomagnesemia. The dose for administration is 1–2 g diluted in 10 mL of fluid given IV/IO over 20 minutes.
Combination of Anti-Arrhythmics
There is no benefit to combining different antiarrhythmics. In fact, this can be hazardous due to the proarrhythmic effects of combinations.
Vasopressin
Like epinephrine, vasopressin also causes vasoconstriction, but through nonadrenergic effects. The 2015 AHA Guideline for CPR and Emergency Cardiac care does not indicate that vasopressin is more efficacious than epinephrine to treat cardiac arrests. (Class IIb, Evidence level B-R). Consequently, vasopressin as a resuscitation medication has been removed from the 2015 update for the algorithm for cardiac arrest in adults. It is also not beneficial for use in combination with epinephrine. (Class IIb, Evidence level B-R).
Atropine
Atropine opposes cholinergic effects with decreased heart rate and AV node conduction. No randomized controlled trials are available to evaluate its use in asystole or bradycardia in cardiac arrest, and there is no good evidence indicating a survival benefit. (Class IIb, Evidence level B). Consequently, atropine is no longer in the cardiac arrest algorithm for adults.
Sodium Bicarbonate
During and following cardiac arrest, there is increased acidemia due to poor perfusion. This is worsened with prolonged cardiac arrest, reduced perfusion, and poor oxygenation. Some studies show sodium bicarbonate may help the acid-base status of cardiac arrest; however, the majority do not show improvement, and some show detrimental effects. Consequently, sodium bicarbonate is not routinely recommended to improve acid-base status. Other therapies that improve oxygenation and tissue perfusion (chest compression and airway management) should be used for this purpose.
Calcium
There is no good evidence supporting the use of calcium in cardiac arrest, and it is not recommended for routine use in this situation. It can be useful if the patient has underlying hyperkalemia.
Fibrinolytic Agents
Fibrinolysis can be used in patients with an acute coronary syndrome or significant pulmonary embolism. CPR does not limit the use of fibrinolytics. However, current evidence does not show a benefit of these medications in refractory cardiac arrest. Thus, fibrinolytics should not routinely be used in cardiac arrest unless there is an underlying thrombotic event leading to cardiac arrest.
Fluid Resuscitation
There is no research looking at fluid resuscitation for cardiac arrest. However, it should be used in hypovolemic patients.
Continued Use of Anti-Arrhythmics
There is no definitive evidence indicating a benefit of continued use of antiarrhythmics as prophylaxis against future VF or pVT. However, some experts suggest continuing the medications for up to 24 hours following the termination of the arrhythmia as this may theoretically reduce recurrence. If a patient has a recurrence of arrhythmias, healthcare providers should evaluate for underlying causes such as ischemic events, abnormal electrolytes, and hypoxia.
Managing the Underlying Cause of Arrhythmia
The most common causes of cardiac arrest are acute coronary syndromes as they trigger arrest from cardiac ischemia. Other causes include hypoxemia, medication-induced arrhythmias, and electrolyte imbalance. Patients with MI may require cardiac reperfusion with fibrinolysis or percutaneous coronary intervention (PCI). For non-MI cardiac arrest, patients may have an underlying trigger for arrhythmias. They may require a cardiology consultation to evaluate for a functional or structural cause.