Potassium
The potassium gradient across the cell membrane is essential for cellular function. Seemingly minimal changes can lead to a significant change in heart excitability and conductivity. Rapid alterations in potassium levels can cause significant arrhythmias and threaten life.
Normal serum potassium is 3.5-5 mEq/L.
Hyperkalemia
Hyperkalemia can lead to life-threatening consequences. There is a range of causes for this condition, including excess cellular release, inability to excrete excess potassium, or administration of excess potassium. A low pH is associated with potassium shift outside of the cells. In contrast, a high pH will cause potassium to return inside the cells.
The most common exogenous etiology is prescription medications, especially potassium supplementation, used to manage hypokalemia. It is vital to recognize the signs of hyperkalemia quickly to manage toxicity.
Diagnosing hyperkalemia
Patients with hyperkalemia will have hypotension, paresthesia, and weakness. As it progresses, flaccid paralysis develops, alongside paresthesia, decreased reflexes, and respiratory paralysis. ECG finding of hyperkalemia can help classify the severity. The initial ECG finding in hyperkalemia is peaking T waves, progressing to flat or lost P waves, a prolonging PR interval, wide QRS, deep S waves and fused S-T wave. At even higher levels, ventricular arrhythmias can develop and progress to critical arrhythmias, including PEA, asystole, and VF or V-Tach.

Hyperkalemia Intervals ECG
Treating Hyperkalemia
Initially, reduce any exogenous potassium ingestion by stopping supplementation and any medications that lead to hyperkalemia. Options to manage hyperkalemia include medications that oppose potassium effects on the cell (i.e., calcium), medications that shift potassium inside the cell (i.e., insulin with dextrose, albuterol, and sodium bicarbonate) and medications that help to excrete potassium (i.e., loop diuresis, hemodialysis, resins).

Insulin is one of the hyperkalemia management options.
For mild (5-6 mEq/L) to moderate (6-7 mEq/L) hyperkalemia: treat by administering medications to help excrete potassium and rapidly shift potassium intracellularly.
- IV infuse 1 mg/kg furosemide (40-80 mg). Monitor for hypotension, hypovolemia, or other electrolyte imbalances.
- PO or PR 15-50 g (in 20% sorbitol) Kayexalate
- Dialysis: particularly in those with renal failure already receiving dialysis
- Insulin and glucose: Combine 10 U regular insulin with 25 g glucose. IV infusion for 15-30 minutes
- 10 -20 mg of Albuterol nebulizer for 15 minutes
- IV 50mEq sodium bicarbonate. Typically, use this in conjunction with insulin and glucose or albuterol.
Severe Hyperkalemia
Patients with hyperkalemia who are nearing arrest often will be in renal failure. Hyperkalemia can also be associated with system-wide acidosis, so these two conditions must be managed concurrently. If potassium levels are above 6.5 mEq/L and there are associated ECG changes, emergent care is required. Management for severe hyperkalemia includes
- Administer calcium
- IV 5-10 mL 10% calcium chloride for 2-5 minutes then
- IV 15-30 mL 10% calcium gluconate for 2-5 minutes.
- Calcium antagonizes potassium at the cellular membrane, decreasing its irritable effect on the heart, particularly decrease the risk for VF.
- Shift potassium into the cells using glucose with insulin, albuterol or sodium bicarbonate
- Excrete potassium from the body using diuresis, dialysis, or resins. Use dialysis if there is renal failure.

Calcium is administered first to protected the cardiomyocytes and does not lower the serum level of potassium.
If cardiac arrest develops, treat the patient according to standard management; however, administer hyperkalemia specific therapy, i.e., calcium and sodium bicarbonate concurrently. (Class IIb, Evidence level C).
Hypokalemia
Significant hypokalemia may occur in the setting of renal and gastrointestinal losses and associated hypomagnesemia. Low potassium will lead to changes in heart excitability and conductivity and leads to specific ECG changes, including U waves, flattening of the T wave as well as arrhythmia, including ventricular arrhythmia leading to PEA or asystole. Hypokalemia may be associated with VF.
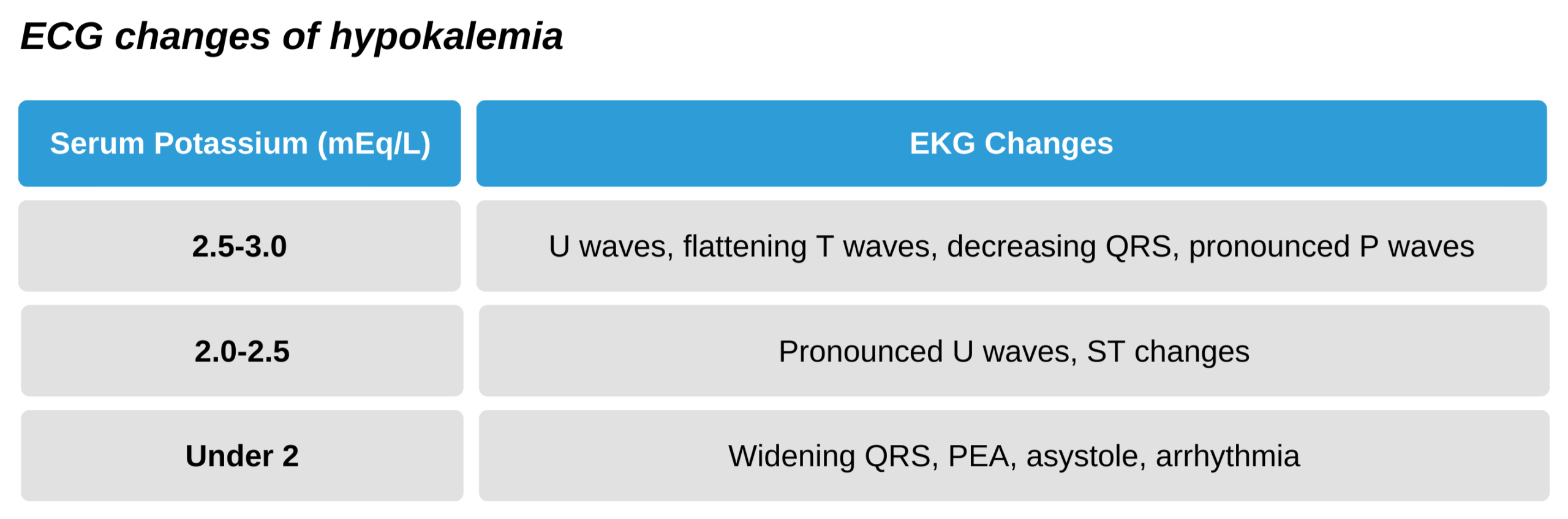

Hypokalemia ECG Changes
Treating Hypokalemia
Do not simply treat hypokalemia associated cardiac arrest with boluses of potassium. (Class III; harmful, Evidence level C).
Mild to moderate hypokalemia
For this level of hypokalemia, the potassium deficit should be calculated and replacement based on this.
- 1mEq/L serum decrease is associated with a body deficit between 150-400 mEq.
- The body potassium and estimate of potassium body deficit depend on patient characteristics, including body size, age, and sex. Male sex and larger body size suggest a higher associated body deficit.
- Remember that pH changes will affect the potassium level. For each 0.1 unit elevation in pH above the normal (pH of 7.45), there will be an associated decrease in potassium by 0.3 mEq/L Consequently, an alkalotic patient will have a lower than expected serum potassium compared to total body potassium and would need less potassium replacement.
- The route and speed of the supplementation of potassium depend on the patient’s condition. With increasing symptom severity or instability, more rapid replacement is needed.
- In clinically stable patients, replace between 10-20 mEq per hour.
- The maximum dose is 40mEq per hour. This will increase serum level by about 0.5 mEq/L.
- Monitor cardiac rhythm during replacement. Ensure the catheter tip is not in the atrium if a central line is used as this can precipitate arrhythmia.