Managing Tachycardias
- The initial management for reentry SVT is vagal maneuvers or adenosine. Vagal maneuvers will treat up to ¼ of reentry SVTs. Adenosine is needed to treat the rest.
- Unstable patients with persistent tachycardia as the cause of their symptoms should be managed with synchronized cardioversion immediately.
- Stable wide-QRS tachycardias should be managed with cardiology consultation.
Related Video: Adenosine – ACLS Drugs
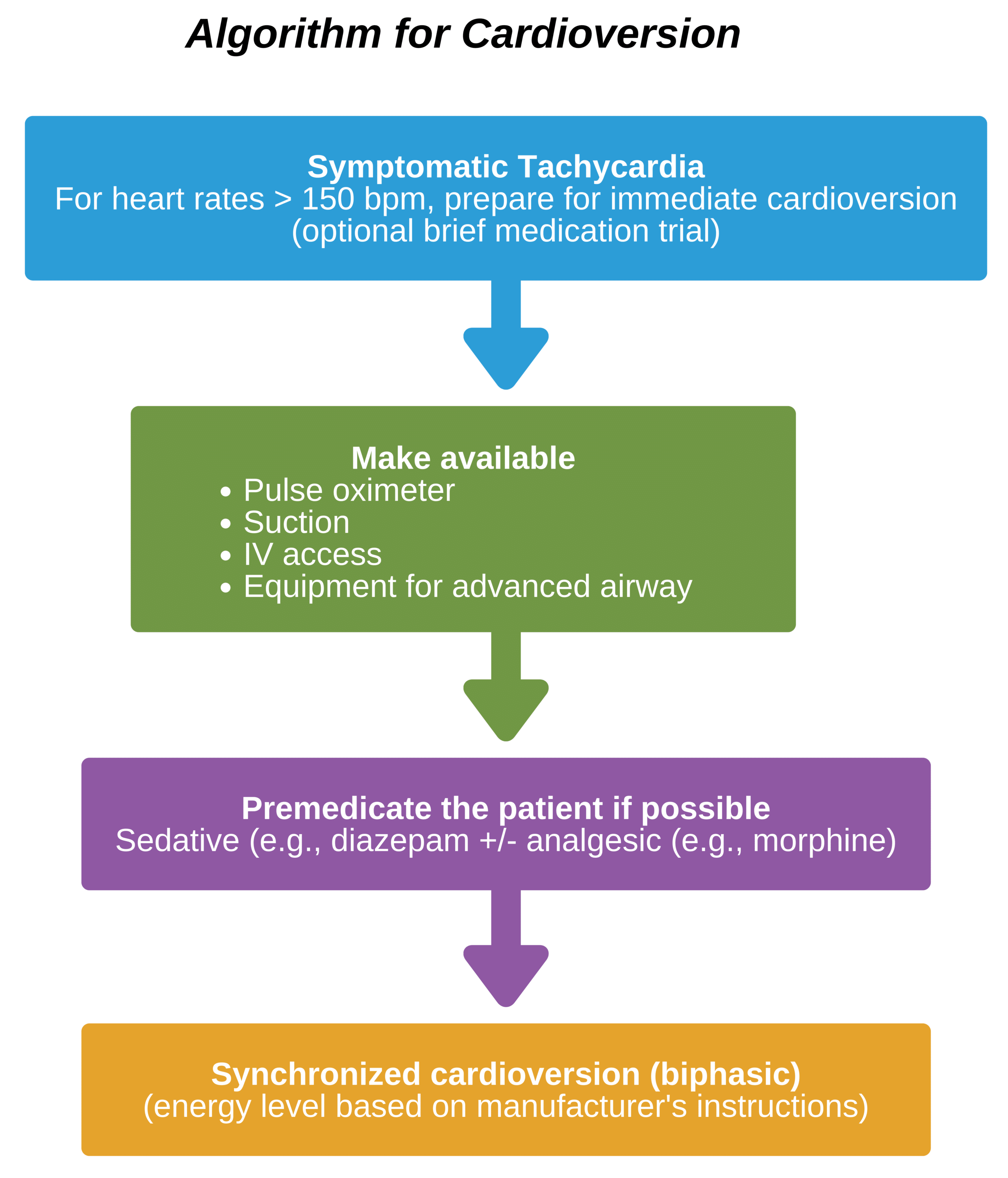
Cardioversion in Stable or Unstable Tachycardia

Cardioversion Pad Positioning
Manage tachycardias with synchronized cardioversion, which times defibrillation to correlate with the QRS. This decreases the chance that defibrillation will occur during the relative myocyte refractory period (or vulnerable period) in which myocytes are at higher risk for VF.
Generally, energies used in synchronized cardioversion are less than in nonsynchronized defibrillation. Shocks using less energy can cause as much pain and have a similar risk of VF as higher energy shocks. Still, they are less likely to lead to bradyarrhythmias or cause injury to tissues. Consequently, lower energies are preferred. However, if not available, nonsynchronized defibrillation can be used.
Related Video: Synchronized Cardioversion for Tachycardia
Reentry tachycardias are unstable or refractory to medications and are excellent candidates for synchronized cardioversion. Such tachycardias are due to depolarization waves that repeatedly circulate, causing an arrhythmia circuit. Examples include atrial fibrillation and flutter, monomorphic VT, and SVTs. A well-timed shock can help stop this abnormal circuit and end the arrhythmia. The 2015 AHA Guideline for CPR and Emergency Cardiac Care recommends defibrillation for arrhythmias of both the atria and ventricles. (Class 1, Evidence level B-NR)
Patients who receive synchronized cardioversion should have IV access as most will be conscious and require sedation. However, if the patient is not stable, a lack of access should not delay cardioversion. It is also important to be aware of the possible adverse effects of synchronized cardioversion, including VF and bradycardia, that may need subsequent treatment.
Defibrillators provide current via either monophasic or biphasic waveforms. Monophasic waveforms push current in mostly one direction. Biphasic waveforms push current in one direction for some time, then switch direction for the remainder of the time. Biphasic defibrillators are more commonly available in the modern era.
The AHA Guideline for CPR and Emergency Cardiac Care states that biphasic defibrillators are preferred for treating atrial and ventricular arrhythmias because of the improved likelihood of stopping the arrhythmia. (Class IIa, Evidence level B-R)
- No data are available to recommend one type of biphasic defibrillator over another. Responders should follow the manufacturer’s instructions to choose the dose of energy for the initial shock. If there are no instructions, the maximal energy dose available should be used. (Class IIb, Evidence level C-LD)
Cardioversion does not manage junctional tachycardias and other tachycardias that have automatic foci arising from cells that depolarize spontaneously. Cardioversion may increase the tachyarrhythmia, worsening the situation.
Key Takeaway
Do not use cardioversion for junctional tachycardias since this may worsen the situation.
If using a biphasic defibrillator, it is recommended to follow the manufacturer’s instructions or use the highest dose available if there are no instructions available. While synchronized cardioversion is the treatment of choice in patients with an organized ventricular rhythm, if this is not available or the patient is unstable, and the diagnosis is not clear, responders should proceed with unsynchronized defibrillation.
Defibrillation Steps in Adults
Assessment of the cardiac rhythm should always be the first step. If VF or pVT, responders should ensure high-quality CPR and limit interruptions to the chest compressions.
Defibrillation in in Tachycardia with a Pulse
- The patient should first be sedated if conscious. If the patient is unstable, the team should proceed immediately.
- The defibrillator is powered on and the manufacturer’s instructions followed for the energy dose to be given. If unknown, the highest energy dose should be used.
- The leads are then attached to the patient, with the team ensuring the patient’s rhythm is appropriately displayed.
- Adhesive pads are then applied to the patient ensuring cables are attached. Less preferred are paddles using conducting gel/paste.
- Pads are placed using anterior-posterior positioning (right anterior and left axillary). The team makes sure pads are away from implanted devices or medicine patches and that there is no oxygen across the chest.
- The defibrillator team member activates the sync control to start synchronization and looks for R wave markers to indicate the device is in sync with the patient’s QRS complex.
- The appropriate energy level is then set according to the manufacturer’s recommendations.
- The defibrillator team member states “charging, stand clear” and presses the charge button.
- When fully charged, the team members clear the patient and state, “All clear!”
- The defibrillator team members presses the shock button.
- Another monitor check is done. If the tachycardia continues, another shock will be given after resynchronizing the device.

Rescuer Holding Defibrillator