Calcium
Imbalances in calcium rarely will lead to cardiac emergencies. Consequently, there are no guidelines for evaluating calcium imbalance during arrest situations. Of course, calcium is used in hyperkalemia and hypermagnesemia related cardiac emergencies. Calcium is the most common body mineral, and the body depends on it for numerous physiological processes. Calcium within the cells is necessary for functions such as muscular and cardiac contraction, receptor activation, and platelet aggregation. It is also necessary for the strength of bone. One half of calcium in the serum is inactivated and bound to albumin, while the rest is active and ionized. Vitamin D and parathyroid hormone regulate calcium levels.
The body calcium level is affected by the albumin level. With every increase in the serum albumin of 1g/dL, the body calcium will rise by 0.8 mg/dL, and vice versa. On the other hand, ionized calcium levels- the active form- will decrease with increased serum albumin levels. In those with hypoalbuminemia, even though total calcium may be low, the ionized calcium can remain normal. It is important to know that routine metabolic panels usually measure serum calcium and not ionized calcium and can miss changes in ionized calcium.
The normal serum calcium ranges from 8.5-10.5 mg/dL, while the ionized calcium ranges from 4.2-4.8 mg/dL.
To determine true calcium (in the setting of hypoalbuminemia) the equation is:
- Calcium true = Calcium measured + [(0.8) x (Protein normal – Protein measured)]
There is more extracellular calcium that intracellular. Both sodium and calcium are excreted from the cell. Calcium opposes the effects of both magnesium and potassium at the cell membrane. It is useful for the management of elevated levels of either ion. Calcium is used for
- Hyperkalemia
- Ionized hypocalcemia (i.e., repeated blood transfusion)
- An antidote for calcium channel blockade
Calcium is controlled rigidly by PTH, which is released from the parathyroid when low ionized calcium occurs. There are three effects of PTH secretion from low calcium:
- A decrease in calcitonin which leads to osteoclast (breakdown) activity in the bone and leads to increased calcium levels;
- An increase in kidney reabsorption of calcium resulting in increased calcium levels;
- Activation of Vitamin D to Calciferol, which increases GI reabsorption of calcium and leads to increased calcium levels.

Calcium Regulation
Hypercalcemia
Excess calcium is usually related to increased release from the intestine or bones or from decreased execration from the kidneys. Symptoms include constipation, dysphagia, and pancreatitis. The kidney will have a reduced ability for urinary concentration leading to the loss of other ions- potassium, sodium, phosphate, and magnesium. There is an attempt to reabsorb calcium, which worsens the problem.
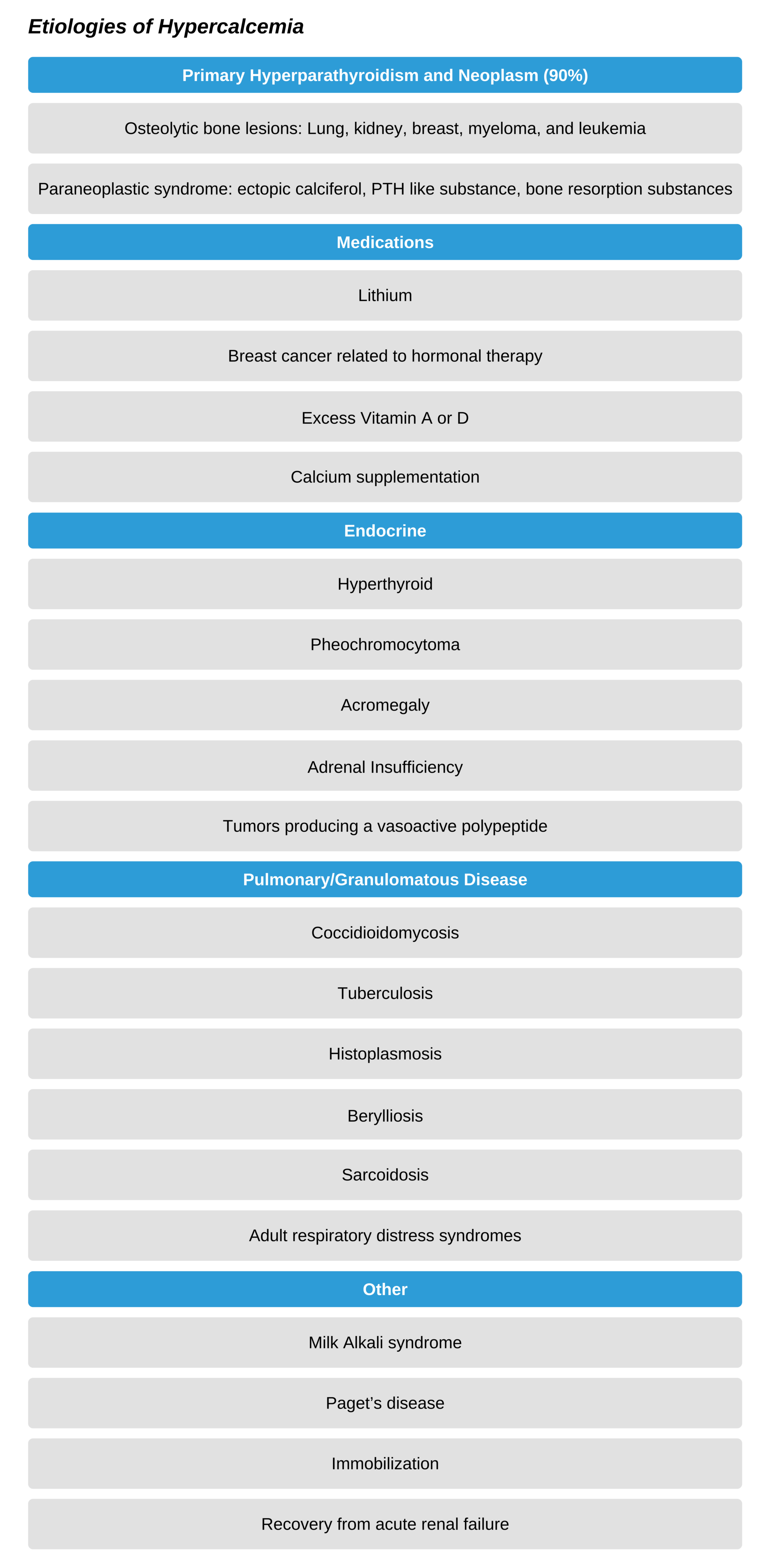
Etiologies of Hypercalcemia
Hypercalcemia is more common than hypocalcemia, with an incidence of between 0.3-6%. It is usually associated with hyperparathyroidism or neoplasm. There are paraneoplastic syndromes in which a substance similar to PTH is released, which causes an excess bone release of calcium. On the other hand, primary hyperparathyroidism usually causes its effect on the intestinal calcium reabsorption.

Parathyroid hormone regulates serum calcium levels.
Diagnosing Hypercalcemia
Symptoms usually begin when total calcium levels are over 12-15 mg/dL. Patients may notice fatigue, weakness, depression, or confusion. At even greater levels (over 15-20 mg/dL), there can be seizures, hallucinations, disorientation, or coma. Due to the diuretic calcium effect on the kidneys, the patient will lose volume with resulting dehydration. Remember the mnemonic, “bones, stones, moans, and psychological overtones”:
- Bones: osteolytic lesions release calcium
- Kidney stones
- Moans: abdominal pain
- Psychological overtones: depression/apathy, coma/stupor, irritability and hallucination
With initial hypercalcemia, there can be increased cardiac contractility. However, when the level is over 15 mg/dL, depression of the myocardium begins with diminished automaticity and shorter ventricular systole. Arrhythmias may occur due to a shortened refractory period. Additionally, hypercalcemia potentiates digitalis toxicity and can lead to hypertension. There can also be hypokalemia, which also increases the risk of cardiac dysfunction. Other cardiac findings include a short QT interval (at above 13 mg/dL) and long PR interval and widened QRS. AV block progressing to heart block, and arrest can occur at levels between 15-20 mg/dL.
Treating Hypercalcemia
Treat symptomatic patients or those with levels over 15 mg/dL. Replenish vascular volume using normal saline and calcitonin plus a bisphosphonate. IF there is both normal heart and kidney function, administer 300-500ml per hour of IV normal saline until the patient has good diuresis (usually 200-300ml/h urine output). Titrate this as needed based on patient characteristics and response. The fluid infusion can be decreased to 100-200 ml/h. Ensure close monitoring of magnesium and potassium as diuresis can lead to losses of these electrolytes as well.
Calcitonin works rapidly to reduce serum calcium as it decreases the amount of resorption of bone and improves renal excretion of calcium. It is rather safe, but not very potent. Bisphosphonates work by blocking the resorption of bone by osteoclasts. Zoledronic acid and pamidronate are two potent drugs used for hypercalcemia. However, as the major effect takes 2-4 days, calcitonin, with its faster onset of action, is given in conjunction.
Dialysis is used to excrete calcium in patients with associated renal or heart failure. Chelation agents such as ethylenediaminetetraacetic acid can be used in severe situations. In cases of associated malignancy, hypercalcemia will progress with tumor progression. Treatment should be in alignment with the patient’s overall treatment plan, prognosis, and wishes, especially in the case of a patient who is actively dying. Recommendations for hypercalcemia management include
- 12-15 mg/dL: treat if symptomatic
- Over 15 mg/dL: treat regardless of symptoms. There are four areas of treatment. The first two will be done in the acute setting, possibly by ACLS providers.
- Volume replacement: 300-500ml per hour of IV normal saline until volume replaced, which increases calcium excretion. Decrease infusion to 100-200ml per hour.
- Eliminate calcium via kidneys:
- saline diuresis leads to 1.5-2.5 mg/dL reduction in calcium levels.
- Consider IV 1mg/kg furosemide, especially for heart failure patients. Ensure adequate volume and note that there may be associated calcium reuptake.
- Replace magnesium (15 mg/h) as well as potassium (as high as 10 mEq/h) as there is often associated electrolyte loss.
- Eliminate calcium via bones: this usually takes hours or longer to work and is therefore not used for acute management.
- Calcitonin blocks bone resorption (opposing osteoclasts) and increases calcium deposition. Its effect is modest.
- Bisphosphonates block osteoclast activity and increase the apoptosis of osteoclasts. Options include zoledronic acid and pamidronate.
- Other treatments include indomethacin, glucocorticoids, oral phosphates, and gallium nitrate.
- Treat underlying disorders: this is unique to the patient and underlying condition.
Hypocalcemia
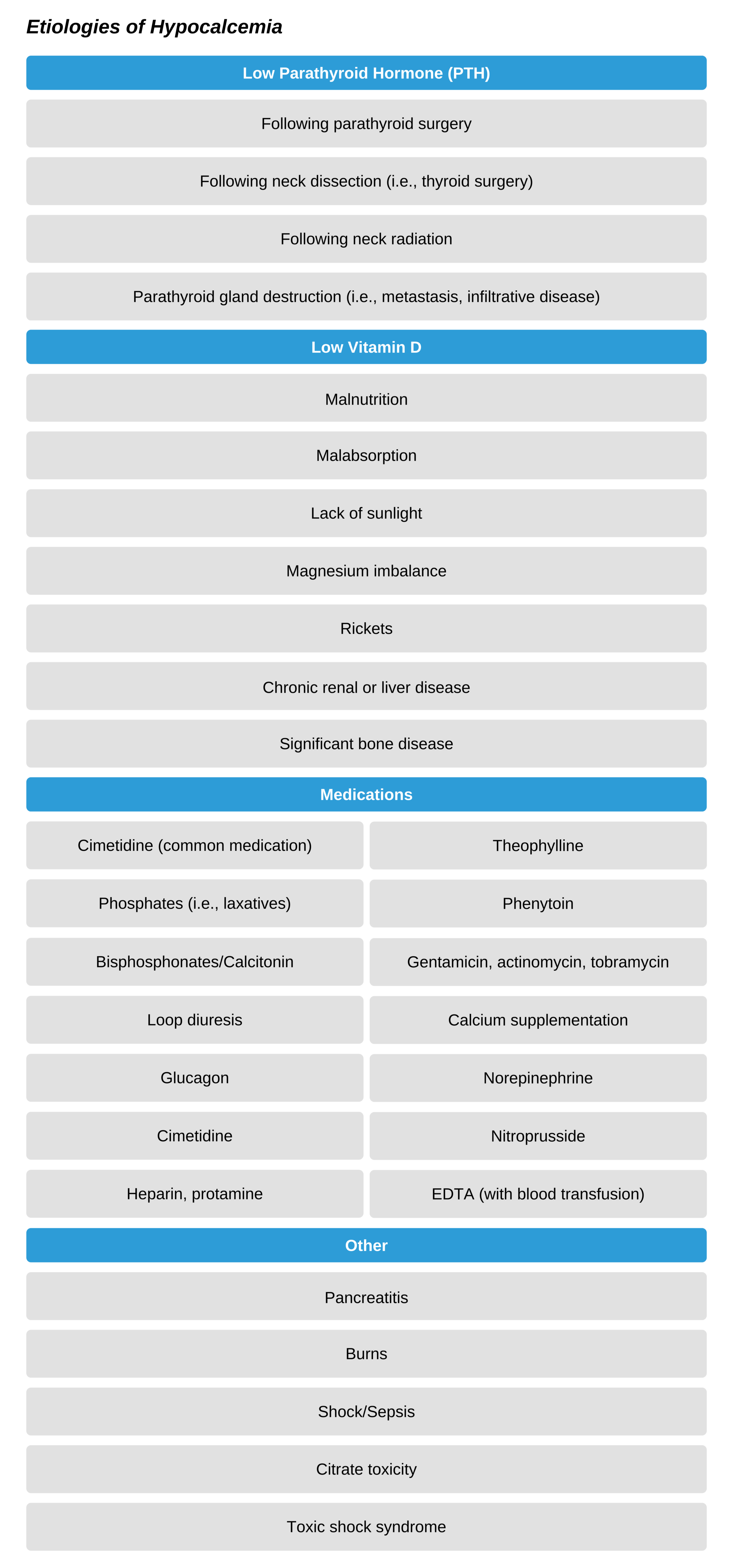
Etiologies of Hypocalcemia
This is less common than hypercalcemia at about 0.6%. It usually is associated with toxic shock syndromes, post thyroid resection, fluoride toxicity, magnesium imbalance, or tumor lysis syndromes (rapid turnover of cells leading to hypocalcemia, hyperkalemia, and hyperphosphatemia). Additionally, common causes include pancreatitis, low vitamin D, and medication complications.
Diagnosing Hypocalcemia
Patients will usually be symptomatic if ionized calcium is below 2.5 mg/dL and will report paresthesia, muscle cramps, then spasms including stridor, laryngospasm, seizures, or coma. There is pronounced hyperreflexia with Chvostek (facial nerve tap causes eyelid or mouth twitch) and Trousseau (spasm of hand/fingers following pressure cuff inflation secondary to ulnar nerve ischemia) sign positive. Cardiac effects, including potentiation of digitalis toxicity, can also occur. ECG will show a long QT interval, T wave inversions, bradycardia, and AV block as well as V-Tach.
Treating Hypocalcemia
Replacement of calcium is necessary. It is also dependent on magnesium and potassium levels, and often the three electrolytes must be managed concurrently. It is also prudent to monitor pH levels. Begin with IV 5-10 mL 10% calcium chloride or IV 15-30 mL 10% calcium gluconate for 2-5 minutes. Be aware that associated hypomagnesemia will make hypocalcemia refractory to treatment, and this electrolyte imbalance must be treated as well.