Pulseless Electrical Activity (PEA)
Any rhythm (except asystole, VF, and pVT) that is not accompanied by a pulse is PEA. It is important to note that many of these rhythms, especially the supraventricular rhythms, are only temporary and easily deteriorate to more detrimental rhythms over time.
PEA is often associated with an underlying and reversible etiology. Consequently, responders must look for these underlying diagnoses early, such as the Hs and Ts. If these diagnoses are missed, PEA can deteriorate, often leading to asystole or an agonal ventricular arrhythmia.
PEA does not always indicate a complete lack of cardiac output. Studies show that, at least initially, there may be enough electrical activity to cause ventricular contractions. Still, these may be too weak to generate a pulse (which requires at least 45–60 mm Hg). These weak contractions may be detected by cardiac ultrasound or intravascular pressure monitoring. These weak contractions have been called pseudo-electromechanical disassociation.
In such cases, early and aggressive treatment is required.

Pulseless electrical activity (PEA) may appear organized, though it is PEA if there’s no pulse.
Treating PEA and Underlying Etiologies
Survival rates from asystole and PEA are not as good as those from VF and pVT. Part of the reason for this is that asystole is often an end-stage rhythm that follows VF that has “burnt out.” Additionally, it can occur following delayed defibrillation. Consequently, immediate resumption of CPR is key.
Responders should review the cardiac rhythm. PEA with a narrow QRS complex is likely to have an underlying cause that is not cardiac in nature. This very well may be a reversible cause that, if treated quickly, can lead to a successful resuscitation.
Related Video: What is PEA?
Efficient diagnosis of underlying etiologies
Determining the underlying cause of cardiac arrest is always a vital task. While some of these diagnoses are discovered in the post-arrest period, such as cardiac arrest due to acute coronary syndrome or ACS, other noncardiac causes need to be identified during cardiac arrest to improve outcomes.
The BLS assessment and initial and secondary evaluations consider the known differential diagnoses to determine the cause of cardiac arrest. This critical evaluation is most important in cases of asystole and PEA, where reversible causes are most likely. In these situations, the Hs and Ts should be at the forefront of the search for underlying etiologies. They should be actively evaluated, ruled out, or identified and treated during resuscitation.
Related Video: Treating Reversible Causes of PEA and Asystole
Hydrogen Ion (Acidosis)
Acidosis is the result of excess hydrogen ions within the blood and tissues, which will lead to loss of the body’s alkaline reserves and a drop in the pH level. ECG findings may include small-amplitude QRS complexes. Patients with severe acidosis may not respond to epinephrine and other adrenergic agonists.
Related Video: Hs and Ts – Hydrogen Ions
Abnormalities in potassium levels lead to electrolyte abnormalities and can affect cardiac function. Both metabolic imbalances, if left untreated, can lead to death.
With hyperkalemia, or elevated potassium levels, the ECG will show T wave peaking and small P waves. An idioventricular rhythm and eventually asystole can occur. For patients with hyperkalemia, there are specific therapies in addition to routine resuscitation efforts. Treatment includes 500–1,000 mg IV calcium chloride or 15–30 mL IV calcium gluconate.
Hypokalemia or decreased potassium levels can show up as flat T waves, obvious U waves, and wide-complex tachycardias. Patients can also develop ventricular arrhythmias and eventually asystole or PEA.
Related Video: Hs and Ts – Hypo-Hyperkalemia
Hypothermia
A decrease in the body’s core temperature to 36 degrees C (96.8 degrees F) or less is the definition of hypothermia. The ECG will show J waves or Osborne waves. In these patients, core warming therapies should be undertaken to return body temperature to normal.
Hypovolemia
A significant decrease in blood volume can cause PEA. In this case, the ECG will initially show tachycardia, and patients may then develop hypotension. As volume continues to decrease, the blood pressure may become undetectable, leading to PEA with a pulse that is no longer palpable.
Patients should be treated and the underlying cause determined. Hypovolemia not related to blood loss, such as dehydration, may require IV or IO fluid replacement. In contrast, blood-loss hypovolemia, e.g., from trauma, may require blood transfusions as well as correction of fluid losses.
Related Video: Hs and Ts – Hypovolemia
Hypoxia
Hypoxia is the result of insufficient oxygen delivery to the tissues of the body. As this happens in the heart, muscle contraction suffers. The patient may also be cyanotic. PEA can be associated with hypoxia, and consequently, advanced airway placement may be needed to achieve sufficient oxygenation.
Related Video: Hs and Ts – Hypoxia
Tamponade (heart)
Cardiac tamponade is caused by pericardial fluid that obstructs the filling of the heart, effectively decreasing cardiac output. The patient will have sinus tachycardia and a drop in stroke volume and, eventually, blood pressure. The appropriate treatment is the evacuation of this pericardial fluid to allow normal filling of the heart and the return of cardiac output.
Evacuation of the pericardial fluid, or pericardiocentesis, is often done in association with cardiac ultrasound in the acute setting. In cardiac arrest, this may need to be performed without ultrasound guidance as prompt treatment is effective. In patients whose tamponade is secondary to trauma, an emergent thoracotomy may be required if pericardiocentesis is not effective.
Related Video: Hs and Ts – Cardiac Tamponade
Tension Pneumothorax
Tension pneumothorax is the result of a chest wound that allows air to enter but not escape the pleural space. Patients may have PEA, VF, or asystole. Often, a patient with tension pneumothorax will be one that is difficult to ventilate with uneven breath sounds and chest rise that is not symmetrical. The treatment is prompt needle thoracotomy and placement of a chest tube.
Related Video: Hs and Ts – Tension Pneumothorax

Tension Pneumothorax in Left Lung
Thrombosis (heart)
Coronary thrombosis is the underlying mechanism for acute coronary syndromes (ACS) or myocardial infarction (MI). The ECG will show changes to the ST segment, resulting in either ST segment elevation MI (STEMI) or non-ST segment elevation MI (NSTEMI). In these cases, the best management is to give cardiac compressions as, while the cardiac pump is no longer effectively pumping, the chambers tend to be filled well, creating a good cardiac output.
When a large MI occurs, PEA can be the result. This generally occurs when the left main or the proximal portion of the left anterior descending artery (LAD) is blocked. In this case, fibrinolytics are not recommended as there have been no demonstrated survival benefits with this intervention in cardiac arrest patients.
Thrombosis (lungs)
Pulmonary thrombosis, also known as a pulmonary embolus (PE), is a cause of cardiac arrest and shock. The sudden obstruction of the pulmonary vasculature leads to an increase in right heart pressures and vasoactive factors that can cause cardiac shock and eventual arrest. Severe or fulminant PE is the most likely cause of cardiac arrest and occurs in about 5% of patients. This severe disease has a high mortality rate of between 65% and 90%. Progression to cardiac arrest can occur within a few hours. Due to the often severe symptoms, patients will usually seek medical care. Patients may have risk factors for thrombosis (e.g., cancer, recent surgery), shortness of breath, and a sudden witnessed arrest. The majority of PE-associated cardiac arrests (36–53%) will present with PEA.

Pulmonary Embolism
Related Video: Hs and Ts – Pulmonary Embolism
Treatment of fulminant PE includes embolectomy (percutaneous or surgical), systemic thrombolysis, and extracorporeal CPR as routine anticoagulation is not sufficient to resolve a massive clot.
Missing image
Managing Known PE
When a patient has cardiac arrest due to a known PE, there are several options for therapy. These include surgical or mechanical embolectomy and systemic thrombolysis. No one therapy is recommended over others, but rather the best option depends on the patient’s circumstances, the provider’s skillset, and the therapies locally available. Thrombolysis may still be used even in a patient who has received chest compressions and other relative contraindications due to the poor survival outcomes from fulminant PE.
Managing Suspected PE
When a patient has suspected PE causing cardiac arrest, thrombolysis can be offered. However, there are no consensus data regarding the criteria for suspected PE nor the recommended dosing, medication, or timing of thrombolytic treatment. Currently, there is no good research regarding the use of surgical or mechanical embolectomy in this patient group.
Toxins
Toxins and drug overdoses can result in PEA. These substances may lead to vascular dilation or cardiac dysfunction and hypotension. Substances have varied effects from severe bradycardia to a prolongation of the QT interval. Due to the wide range of signs and symptoms, patient history is of paramount importance.
Since toxic exposure or drug overdose can progress quickly, management should be swift. On the other hand, depending upon the half-life of the toxin and how much was ingested, symptoms may be temporary as the effects wear off. Consequently, support measures are key, including:
- prolonged CPR
- transcutaneous pacing
- management of electrolyte derangements
- dialysis
- specific antidotes
- cardiopulmonary bypass
- intra-aortic balloon pump
Cardiac Ultrasound
There is some evidence of a benefit of utilizing cardiac ultrasound or echocardiogram in diagnosing and managing cardiac arrest from conditions such as PE, cardiac tamponade, MI, and dissection of the aorta. Both transesophageal and transthoracic ultrasound can be used in these situations. Multiple prospective research studies discovered that there was a greater risk of fatality when ultrasound could not detect cardiac movement.
Consequently, ultrasonography can be used to diagnose certain underlying reversible causes of cardiac arrest, such as tamponade, pneumothorax, and fulminant PE, as well as manage them. Additionally, ultrasonography can evaluate vascular volume, cardiac masses, poor cardiac wall motion, and the contractions of the left ventricle. With a skilled ultrasonographer, these conditions can be diagnosed rapidly, increasing patient survival.
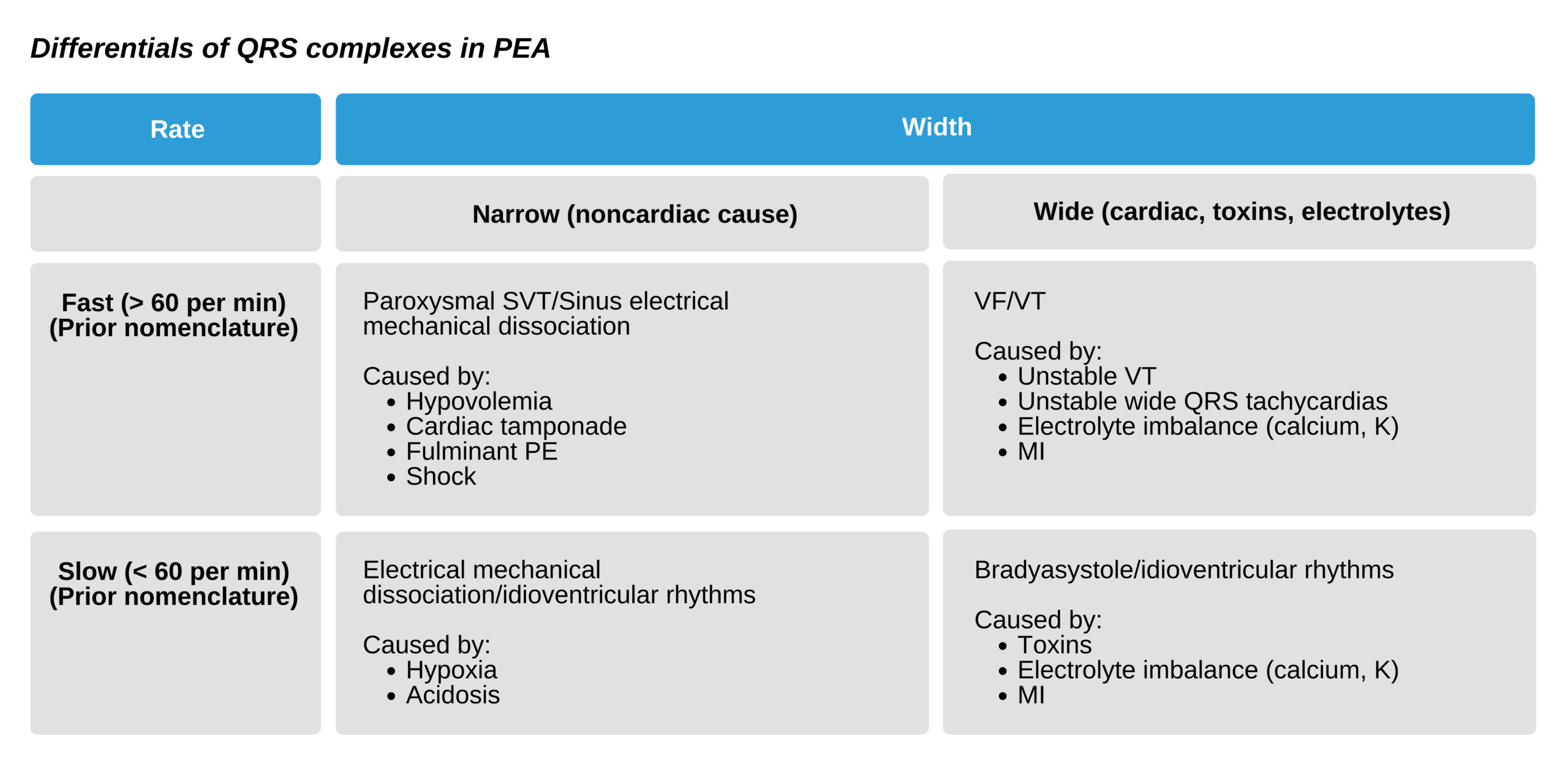
ECG Clues to Underlying Etiologies
The rhythm associated with PEA can be valuable in determining its underlying etiology. Specifically, the QRS complex can provide certain insights: a wide QRS with a slow rate is associated with worse outcomes. This is because these rhythms are associated with cardiac dysfunction, such as the effects from a large MI, and may be the last electrical effort of dying myocytes. On the other hand, certain reversible causes of PEA, such as hyperkalemia, hypoxia, hypothermia, and certain drug overdoses, can also lead to a slow and wide QRS.
A fast and narrow QRS is often associated with relatively preserved cardiac cells and may indicate noncardiac causes like hypovolemia, pulmonary embolism, or sepsis.