Defibrillation Principles
Defining Defibrillation
The most common survivable cardiac arrest arrhythmia is VF. Reducing the time until the patient receives defibrillation increases the likelihood of survival, as this is the best chance for stopping the aberrant rhythm.
When the provider defibrillates a cardiac arrest patient, an electrical current goes through the chest muscles into the heart to stop all cardiac electrical activity and end VF. The electrical shock is delivered to the patient in a controlled manner. When it occurs in synchrony with a cardiac rhythm (atrial fibrillation/flutter or ventricular tachycardia with a pulse), it is often called synchronized cardioversion. Some patients may have a defibrillator implanted if they are at high risk for arrhythmias. These are called implantable cardioverters-defibrillators (ICDs).
Regardless of the type of defibrillator, all of these devices provide a large amount of electrical energy to the cardiac muscle over a short amount of time (milliseconds). By doing so, the defibrillator temporarily stops all cardiac activity, causing asystole. After this moment of rest, the hope is that the cardiac pacemaker cells recover and spontaneously incite coordinated cardiac activity and a normal heart rhythm. This occurs if the cardiac cells are not damaged.
Ensuring Defibrillation Success
Research supporting early defibrillation
Success in cardiac arrest patients with pulseless ventricular tachycardia (pVT) or VF is dependent on early CPR with few interruptions. Additionally, defibrillation should occur as soon as possible. Research supports that this saves lives because:
- Cardiac arrest arrhythmias outside of the hospital are often VF
- Pulseless VF often changes into VF
- VF does not allow the heart to pump blood effectively
- The best VF treatment is early defibrillation
- Defibrillation is more likely to be successful the earlier it is administered
- VF changes into asystole if not effectively treated
Early defibrillation leads to a higher survival rate. While CPR provides a minimal amount of cardiac output, it cannot stop VF and restore a normal heart rhythm. Instead, early CPR in association with defibrillation within minutes of cardiac arrest is needed to restore a perfusing cardiac rhythm. In general, the AHA guidelines suggest that a single shock can be used to defibrillate VF and pVT.
Research indicates that for each minute increase between the time of witnessed VF cardiac arrest and defibrillation, the patient’s chance of surviving decreases 7–10% when no CPR is given. On the other hand, CPR increases the patient’s chance of survival by 3–4% each minute. Overall, early CPR with defibrillation will double or even triple the chance of patient survival. When the general population has access to and uses AEDs, this increases the chance that both CPR and defibrillation will be attempted.
The difference early defibrillation makes
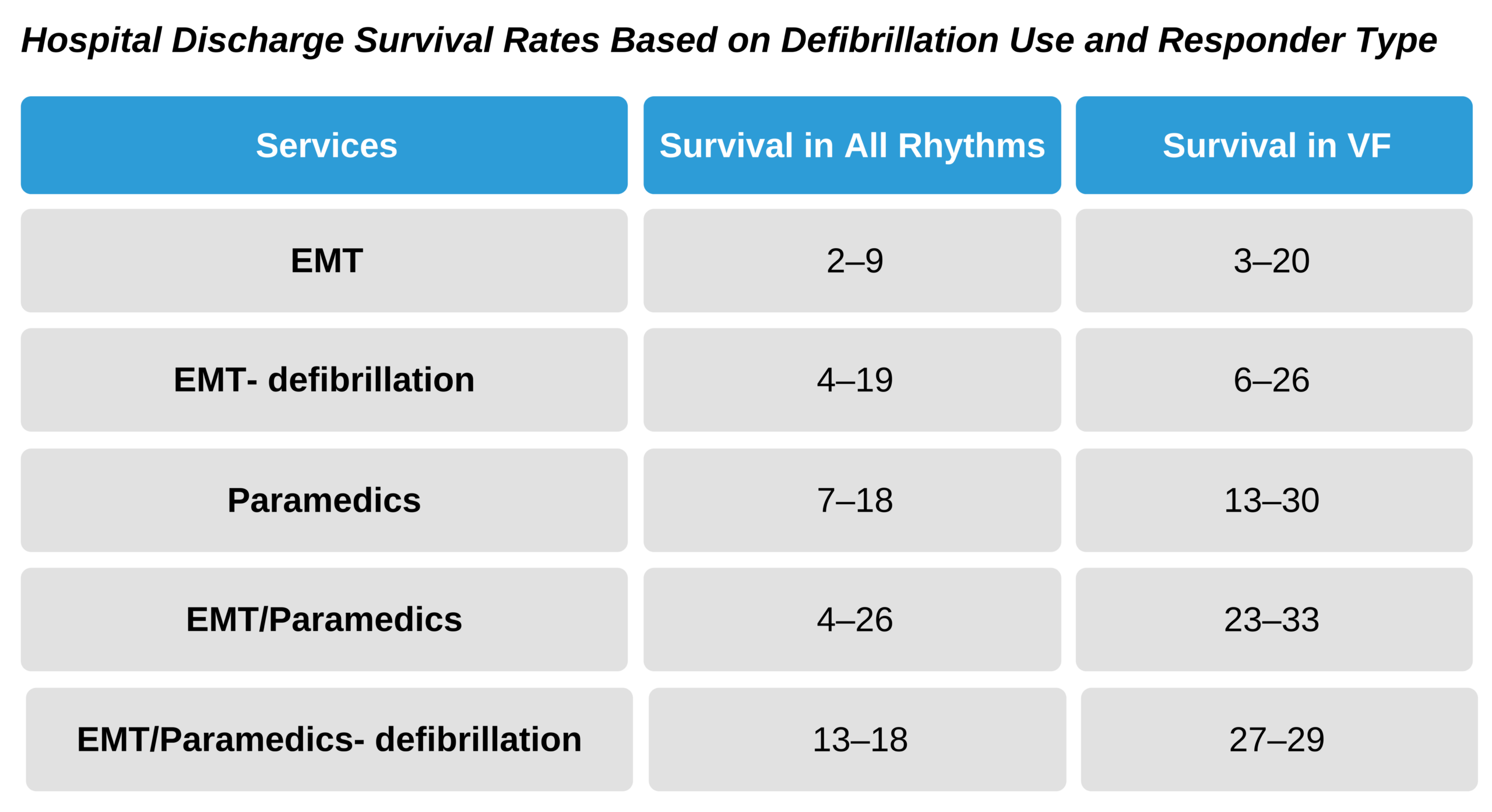
During the 1980s, many communities did not have established ACLS services outside of the hospital. As these services became available in the prehospital setting, studies were conducted to determine the difference made by ACLS and defibrillation before admission to the hospital.
Not surprisingly, EMS noted increased patient survival rates whenever these programs were introduced into the communities. One important example was in King County in Washington state. Studies conducted during the decade showed an odds ratio of 3.7 for survival with out-of-hospital early defibrillation compared to survival without it. There were even higher odds ratios in other more rural communities. In essence, there was an up to six times greater likelihood of surviving with early defibrillation.
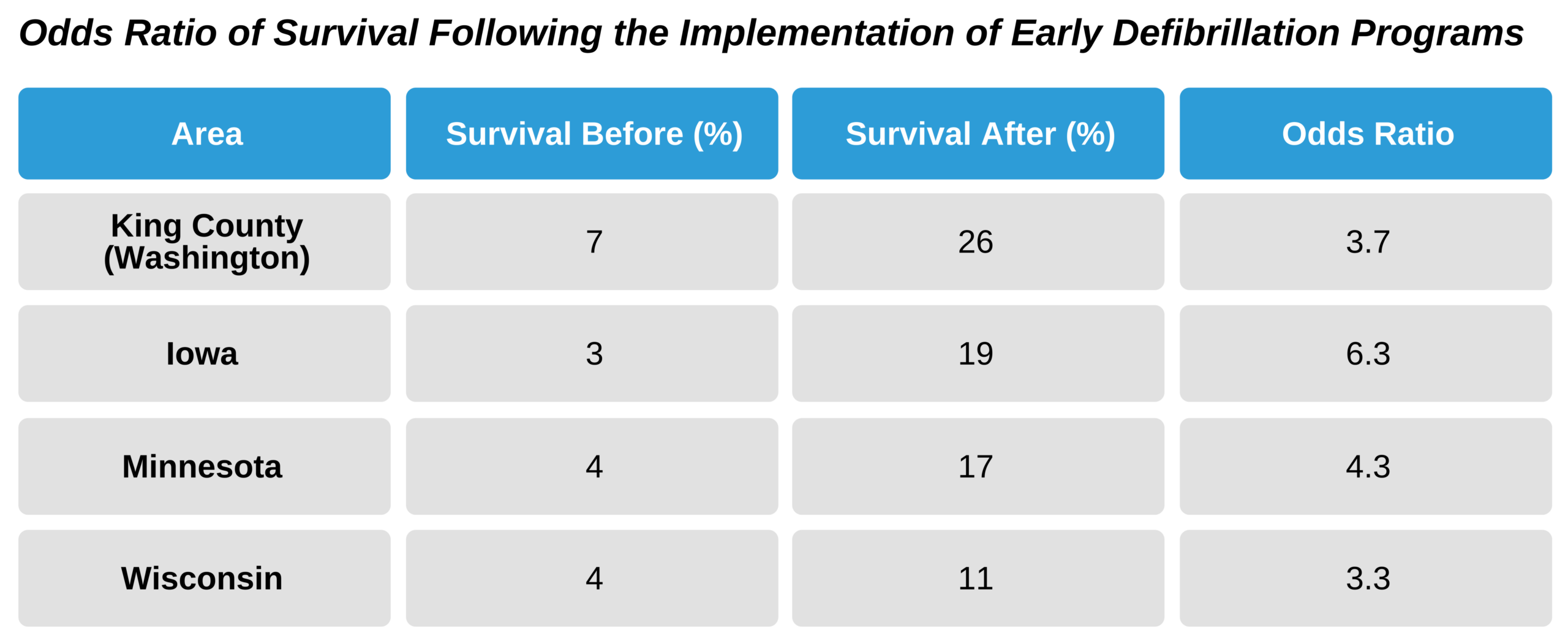
Cummins RO. From concept to standard of care? Review of the clinical experience with automated external defibrillators: percentage of patients with VF surviving before and after implementation of early defibrillation. Ann Emerg Med. 1989;18(12):1269–1275.
Eisenberg MS, Horwood BT, Cummins RO, Reynolds-Haertle R, Hearne TR. Cardiac arrest and resuscitation: a tale of 29 cities. Ann Emerg Med. 1990;19(2):179–186.
These findings were reproduced across the country and showed that early defibrillation was more important than ACLS procedures like advanced airways and IV drugs for improving survival in patients with cardiac arrest arrhythmias. The verdict was in by the end of the decade, and the evidence confirmed that each chain of survival link was valuable with early defibrillation, specifically within 4–5 minutes after the arrest, causing the greatest improvement in survival.
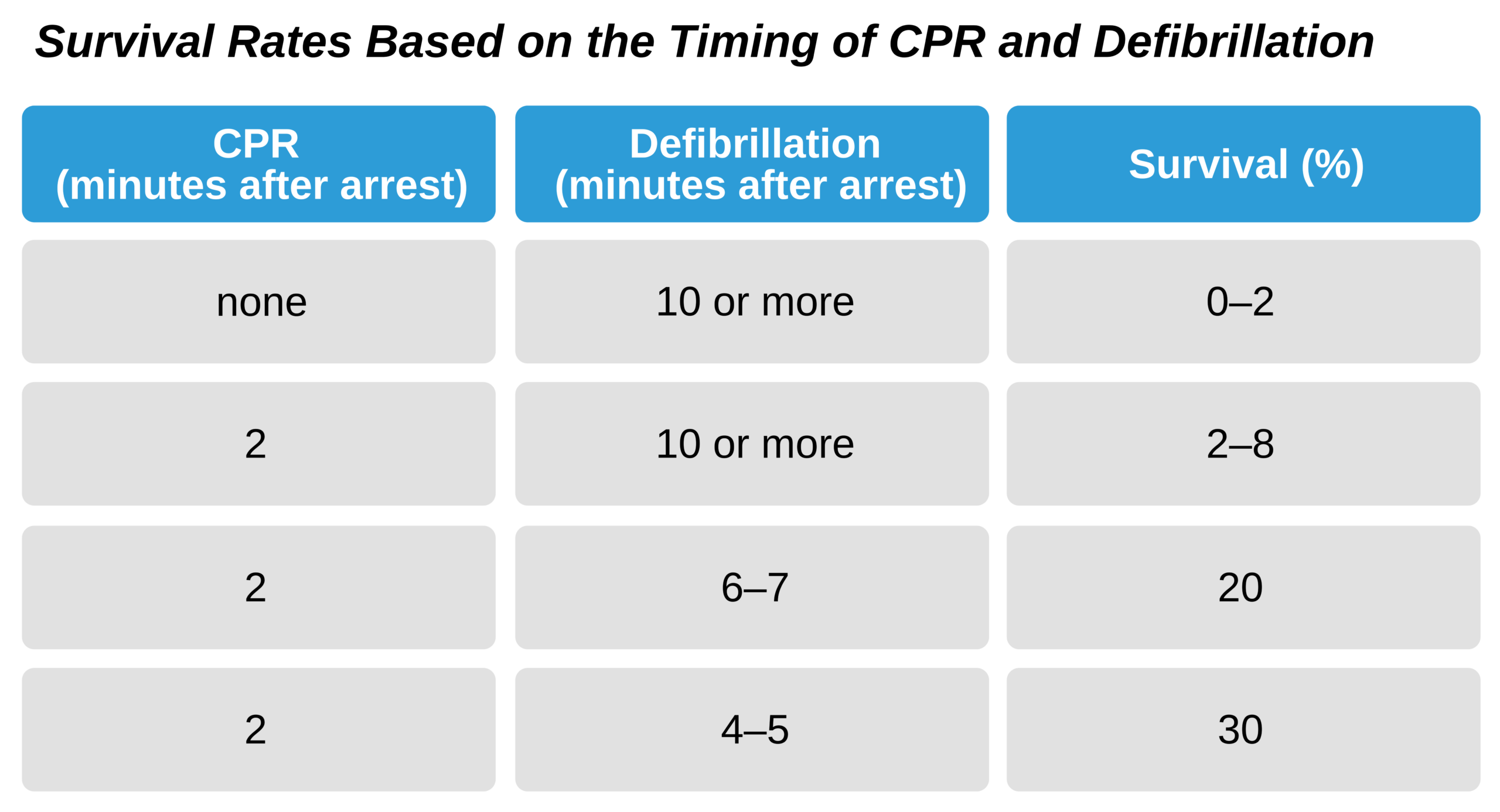
When the responder provides these three components early, survival rates up to 30% are reported by EMS. Additionally, some studies show that cardiac arrest patients with VF treated outside of the hospital with CPR and early defibrillation within 3 to 5 minutes may have survival rates between 41% and 74%.
Key Takeaway
Three vital actions in cardiac arrest to improve survival rates:
- Activate the Chain of Survival
- Provide high-quality CPR
- Defibrillate as soon as possible.
Time is Survival
All studies reveal that early intervention, or time, is the most important factor contributing to improved survival. The best survival rates occur in witnessed cardiac arrest in cardiac rehabilitation settings in which defibrillation usually occurs within 1 minute following arrest. These patients have survival rates that are about 90%.
Additionally, CPR is important, as chest compressions delay the loss of all cardiac function, allowing a longer window for defibrillation to be effective. Generally, if defibrillation is performed between 5 and 10 minutes after arrest in a patient who is getting CPR, the patient is more likely to survive with maintained brain function than one who did not receive CPR.
Cardiac Arrest in Three Stages
There are three stages of cardiac arrest: the electrical, the hemodynamic, and the metabolic phases. Generally, defibrillation is best during the electrical phase. The hemodynamic stage is based on the amount of cardiac output and perfusion to the brain and heart. During this phase, chest compressions can be useful in providing a small amount of cardiac output. The metabolic phase occurs when energy substrates—particularly adenosine triphosphate (ATP)—are used up. During this stage, cardiac damage is most likely to occur.
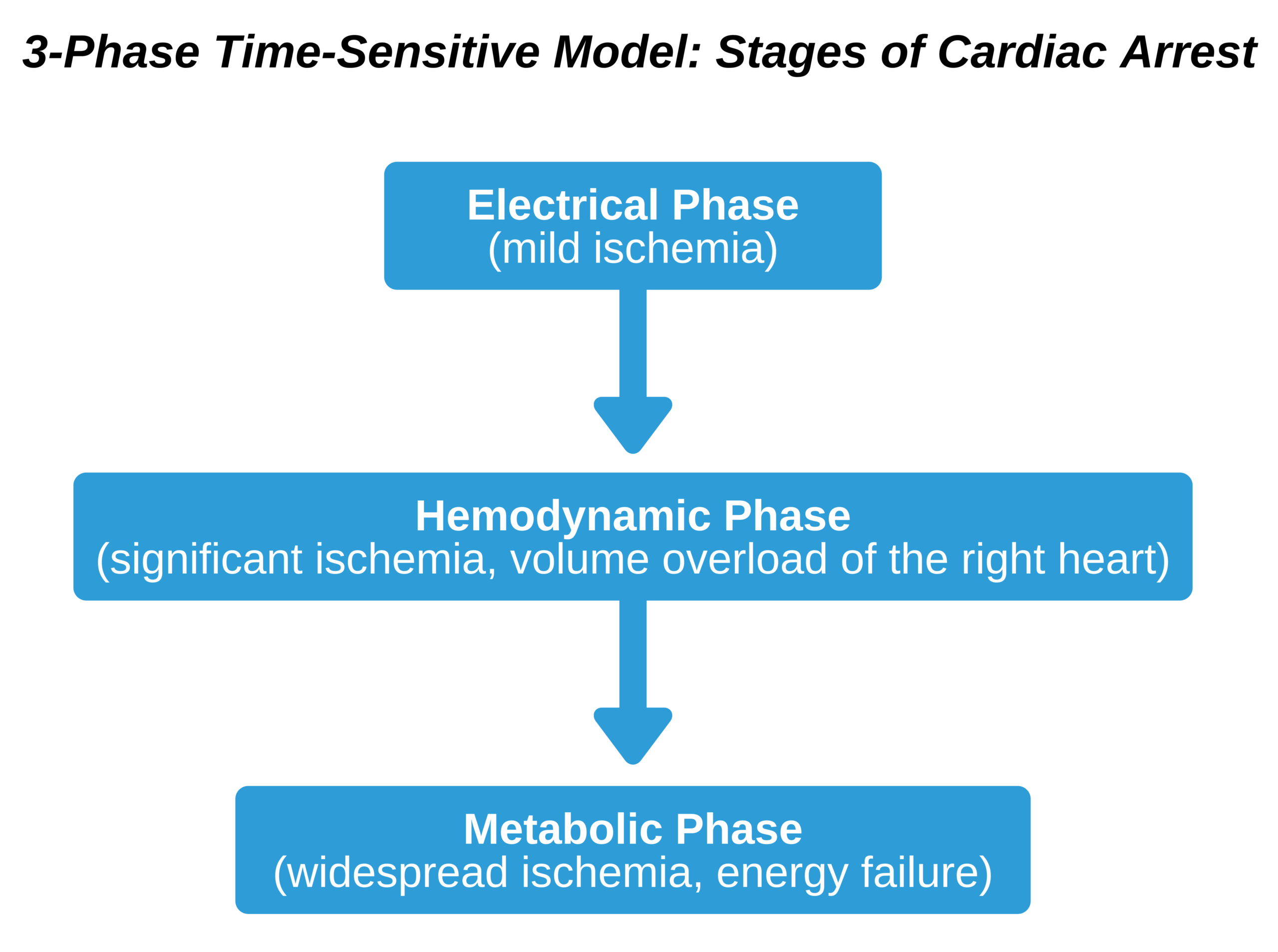
Weisfeldt ML, Becker LB. Resuscitation after cardiac arrest: a 3-phase time-sensitive model: stages of cardiac arrest.
JAMA. 2002;288(23): 3035–3038.
Defibrillation success depends on these stages, as well as the electric and metabolic function of the heart muscle. Also important is the prior heart function and the cause of arrest.
Key Takeaway
The most important factor in recovery from VF associated cardiac arrest is the time between collapse and defibrillation.
Generally, VF is more metabolically demanding than sinus rhythm. Consequently, prolonged VF will deplete the heart’s metabolic stores, such as ATP. This is important because if defibrillation occurs after this point, then there will be no energetic ability to resume normal spontaneous contractions. At this point, defibrillation may lead only to asystole, rather than a perfusing rhythm. This asystole can be permanent. This is why the time to defibrillation is so important.
VF: Shock vs. CPR
Generally, responders should start CPR then defibrillate as soon as it is available. This applies to responders:
- treating cardiac arrest in a hospital or healthcare setting when an AED is immediately available
- treating cardiac arrest outside of the hospital when an AED is immediately available
Providing immediate CPR and early defibrillation during the electrical stage increases the patient’s chance of survival. However, there are no good data that indicate whether defibrillation should be delayed to provide CPR in a patient with VF or pVT outside of the hospital. Generally, if there are two responders, one should begin CPR while the other readies the AED or defibrillator.
Related Video: One Quick Question: Should you Choose CPR or Defibrillation?
When an arrest outside of the hospital is not witnessed, the AHA guidelines recommend 2 minutes of CPR followed by cardiac rhythm analysis. This will provide five CPR cycles with 30 chest compressions and 2 breaths each. Due to the delay of responders arriving to treat these groups of patients, many will likely be in the hemodynamic or metabolic stage of the arrest. Consequently, this CPR may help to make the heart more favorable to receiving defibrillation.
Key Takeaway
In a witnessed cardiac arrest (in or outside of the hospital), start CPR immediately and provide defibrillation as soon as possible.
In an unwitnessed cardiac arrest, provide 2 minutes of CPR before analyzing the cardiac rhythm and defibrillating.
Some studies show that, in cardiac arrest patients with VF who had a delay in treatment of 4–5 minutes or greater, initial CPR of about 2 minutes before defibrillation increased the likelihood of successful resuscitation, survival to hospital discharge, and survival to 1 year.
However, other studies show no difference in survival based on whether defibrillation was delayed for CPR.
It is interesting to note that as the AED became more easily accessible, survival from cardiac arrest surprisingly fell. It is thought that this is because there was less emphasis on high-quality CPR.