The Rapid Assessment
Three simple questions can help to rapidly assess the newly born: Term gestation? Good tone? Breathing or crying? If the answer to all three questions is “Yes,” then the newly born can stay with the mother for routine neonatal care during which the infant is dried, placed in skin-to-skin contact on the mother’s chest, and covered with dry linen or a blanket to maintain a normal temperature.
If the answer to at least one of the questions is “No,” then the infant is moved to a radiant warmer, and the initial steps of neonatal resuscitation commence.
Assessing the Gestational Age
Knowing whether a baby is at term is an important predictor of resuscitation needs. Since a preterm infant has immature lungs and cannot maintain a normal body temperature, the preterm baby often requires more interventions during the transitional stage. Some late-preterm babies may exhibit vigorousness. Thus, they can undergo routine care, and DCC may be an option while the neonatal team performs the initial steps.
What if the newly born child’s gestational age is unknown? Experience and some clinical tools help the team determine if a newly born is at term. The most common tool used to assess gestational age is the Ballard Maturational Assessment Score or, simply, the Ballard Score.
The Ballard Score is calculated by scoring the baby on twelve parameters. A score > 35 denotes that the newly born is a term gestation of at least 38 weeks. If the newly born has a Ballard score < 35 points or appears to be less than 37 weeks gestation, the infant is transported to the radiant warmer after delivery for the initial steps in neonatal resuscitation.
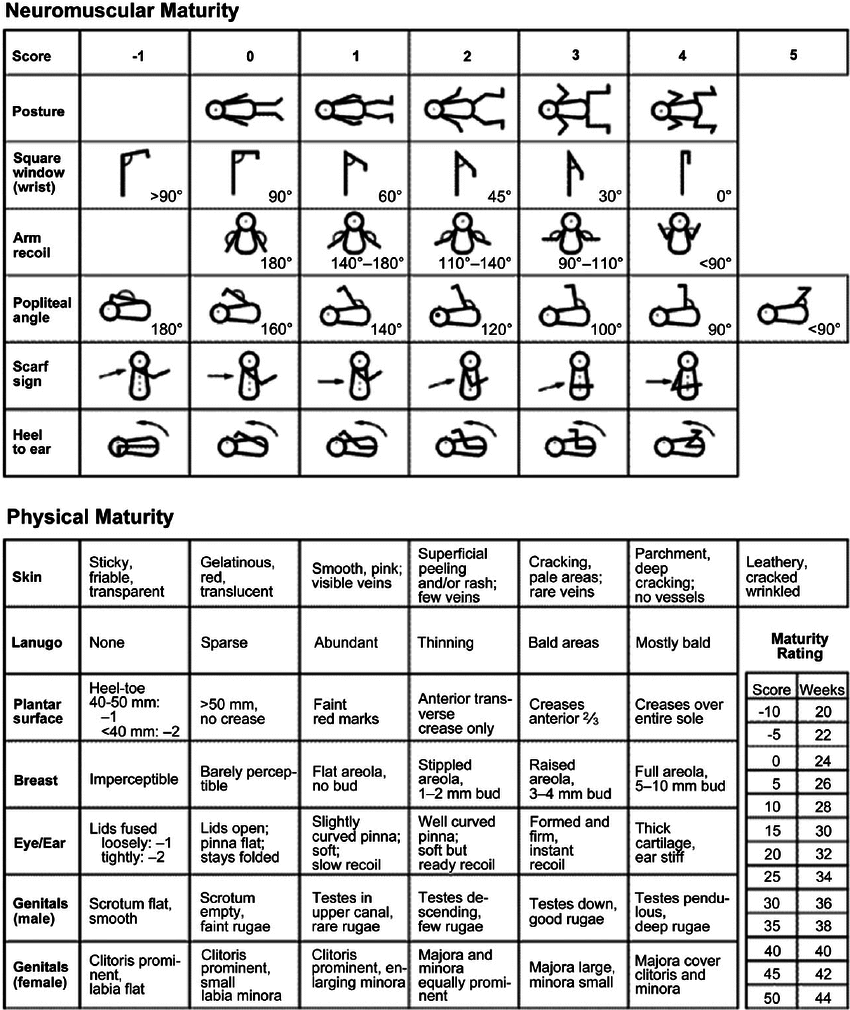
Posture
The most critical parameter to evaluate in the initial assessment is the neonate’s muscle tone. Muscle tone is assessed by looking at the infant’s posture at rest when in a supine position. A preterm infant is increasingly flaccid and resists flexion of the extremities. Flexion in the arms and legs increases with maturity until it becomes the preferred state.
Square Window
This assessment evaluates wrist flexibility by measuring the angle of flexion at the wrist when the hand is bent down toward the forearm. In an infant at full term, the clinician can flex the wrist to the forearm. The angle between the wrist and forearm increases with increased prematurity.
Arm Recoil
Since the term infant naturally prefers flexion of the arms, a rapid arm recoil evaluation can help assess the approximate gestational age. In this exam, the clinician flexes the arm at the shoulder and then quickly extends the arm and releases it. The arm of the preterm infant will not recoil back to a flexed position. The infant at term will exhibit arm recoil.
Peritoneal Angle
In this test, the clinician flexes the infant’s hip up so that the thigh touches the neonate’s abdomen. The clinician then extends the leg at the knee until they feel resistance to the movement. The preterm infant will not resist the extension of the lower leg, but the term infant will resist before the lower leg is at a 90-degree angle to the abdomen.
Scarf Sign
The Scarf sign is elicited by gently pulling or pushing the infant’s arm across the chest. An infant born at term resists this movement before the elbow moves too far across the chest. A preterm infant will not show any resistance to this movement.
Heel to Ear
In this test, the clinician flexes the infant’s leg at the hip to move the heel to the infant’s ear. The severely preterm infant will not resist this movement. The closer to term the infant is, the more they will resist this movement.
Skin
The skin of a term infant will be dry, wrinkled, cracked, and may also be peeling. The skin of the preterm neonate will be “thin.” The very premature infant may have transparent skin that might even stick to the clinician’s fingers.
Lanugo
Lanugo is fine hair that may cover the infant’s body. The clinician should examine the neonate’s back when looking for lanugo. In the severely preterm infant, lanugo may be sparse. As the infant matures, the lanugo becomes more abundant, but it will be patchy or almost nonexistent as the infant approaches term.
Plantar Surface
As the fetus matures in utero, creases begin to appear on the plantar surface of the foot. In the severely preterm infant, there will be no creases on the sole. In the term infant, creases will appear on the entire sole.

Creases on the sole of the infant’s foot (plantar surface).
Breast
In the preterm infant, the clinician will not see the areola or the nipple. In the term infant, the clinician will see a full areola and a breast bud.
Eye and Ear
As the fetus matures, the cartilage in the ear begins to develop and gradually becomes thicker. In a preterm infant, the pinna of the ear is very slow to snap back when it is bent forward. In term infants, the cartilage is stiff and snaps back quickly.
The eye assessment involves the clinician gently separating the eyelids of one eye. The immature infant will have slightly fused eyelids. This evaluation is less predictive of gestational age than the ear evaluation.
Genitals
The preterm male has a smooth, flat scrotum without evidence of descended testicles. As the fetus matures, the scrotum fills out, and rugae begin to develop. In the average term infant, the testicles are descended.
The preterm female has an enlarged clitoris and flat labia. As the fetus matures, the clitoris becomes less prominent, and the labia become more fully developed.