Managing the Newborn with Airway Obstruction
Meconium, blood, mucus, or vernix are common sources of obstruction. Sometimes, congenital anomalies cause anatomic obstructions. If PPV is ineffective, the provider performs the corrective ventilation steps.
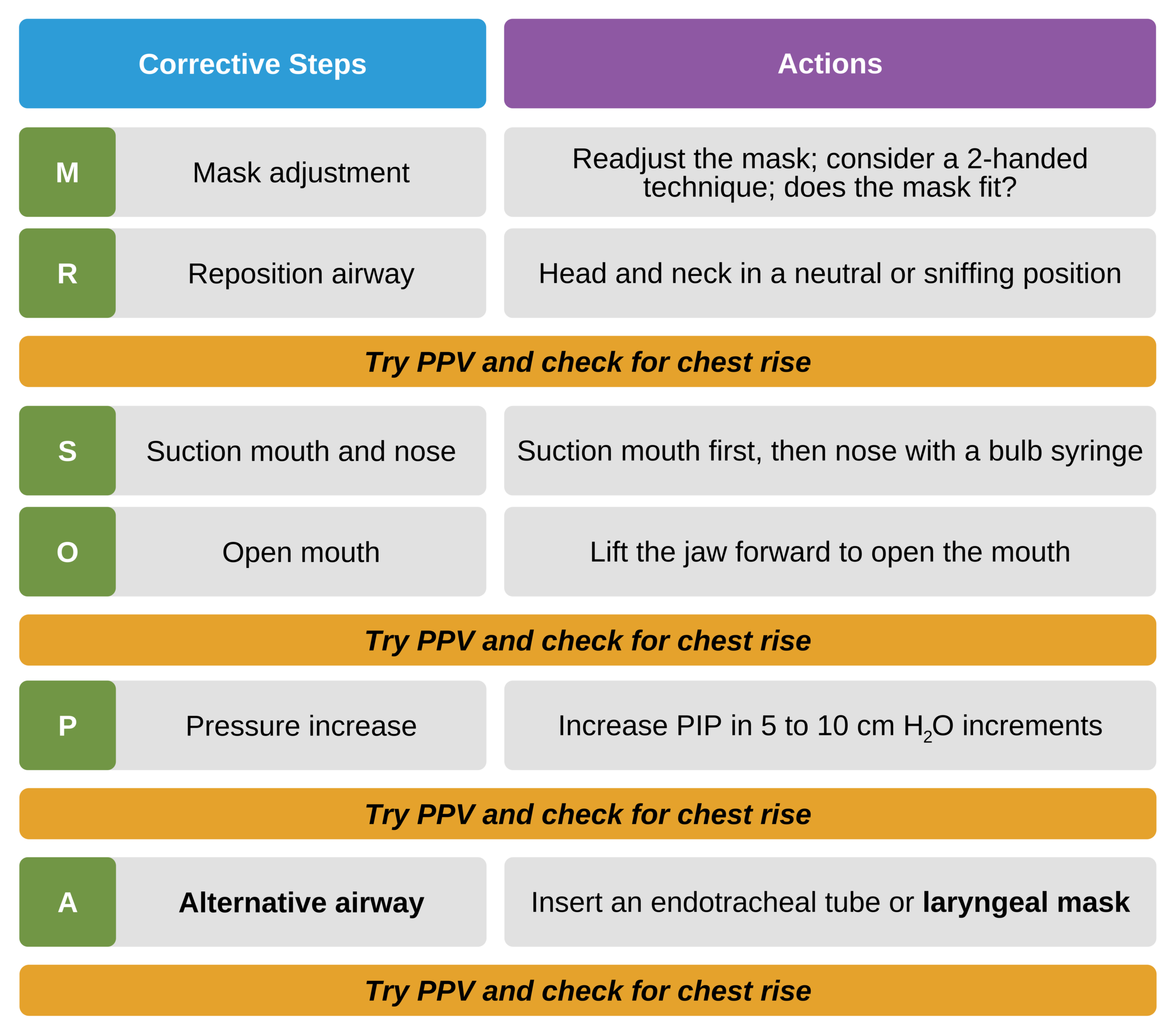
If there is still no visible chest rise after repositioning the mask and the baby’s head and neck, there may be an obstruction in the trachea. Suctioning is the third corrective action step in the MR. SOPA mnemonic and was covered in detail in Chapter 7.
Suctioning the trachea is done through an endotracheal tube using a 5F–8F suction catheter (size depends on the ET tube size). For particularly thick secretions, a meconium aspirator can be attached to the ET tube. A vacuum pressure of 80–100 mm Hg is needed. When using the meconium aspirator, it may be necessary to withdraw the tube gradually to remove the obstruction. The baby is then reintubated with another ET tube after suctioning with the meconium aspirator.
Chest compressions should not be initiated until the clinician is sure the airway is patent.
Anatomic Obstructions Secondary to Congenital Defects
Robin Sequence
Robin sequence is a common congenital anomaly that potentially causes obstruction of the infant’s airway. The baby with Robin sequence has an underdeveloped mandible that is positioned posteriorly compared to the maxilla. This enables the tongue to fall posteriorly, obstructing the pharynx. Cleft palate is a common finding in babies with Robin sequence.

Infant with Robin Sequence.16
Gently turning the newborn into the prone position moves the tongue anteriorly and opens the airway. If positioning is unsuccessful, it may be necessary to place a 2.5 ET tube until the tip is deep into the pharynx just above the larynx. This is a blind procedure and does not require a laryngoscope.
If this does not resolve the obstruction, intubation and PPV may be required. If the baby is difficult to intubate, a laryngeal mask can be used.
Choanal Atresia
Choanal atresia is a congenital abnormality in which the nasal airway is obstructed by bony growth. Newborns naturally breathe through the nose. Hence, this bony growth can cause an airway obstruction unless the infant is crying and breathing through the mouth.
Babies with choanal atresia present with episodes of airway obstruction, cyanosis, or oxygen desaturation, particularly when they are sleeping or breastfeeding. Symptoms spontaneously resolve when they are crying.
Respiratory distress is more pronounced if the choanal atresia involves both nostrils. PPV through a mask is still an effective intervention.

Infant airway with choanal atresia.17
Congenital Diaphragmatic Hernia
Congenital diaphragmatic hernia (CDH) is a defect in the diaphragm that allows entry of the abdominal contents into the thoracic cavity, causing compression of the lungs and other mediastinal structures. It can involve the stomach, intestines, and liver. Restriction of the lung by the presence of these organs hinders lung development. The left side is the most commonly affected site for a CDH.
CDH may be detected before birth during a routine ultrasound. The obstetrician must plan the delivery in an institution with the equipment, expertise, and experience to manage CDH.

X-ray of infant with left-sided congenital diaphragmatic hernia.
Babies born with CDH present with a scaphoid-shaped abdomen, a sign that the gastrointestinal organs have been displaced. They also present with respiratory distress and hypoxemia. The restriction of the mediastinal structures makes CDH patients prone to pulmonary hypertension, which further worsens hypoxemia.
Providing PPV via mask exacerbates the restriction of mediastinal structures as gas can enter the stomach and intestines, increasing its mass effect. Therefore, immediate endotracheal intubation at birth is necessary. After intubation, a double lumen stump-tube, also known as a Replogle tube or an orogastric catheter, size 10F, can be used to decompress the air inside the stomach.

Infant with an orogastric catheter in place.
Pulmonary Hypoplasia
Any clinical condition that restricts the lungs in utero hinders them from developing normally. Pulmonary hypoplasia can result from a space-occupying lesion or severely decreased amniotic fluid (oligohydramnios). CDH and the absence of fetal kidneys also contribute to pulmonary hypoplasia.
At birth, babies with pulmonary hypoplasia present with a small, bell-shaped thorax. If oligohydramnios is a cause, the baby may have other malformations of the hands, feet, nose, or ears. The lack of amniotic fluid restricts the fetal growth of these structures and the lungs in utero.
Inflating the lungs of these patients may be difficult. A higher than usual inflation pressure is often necessary, but it may cause volutrauma. If pulmonary hypoplasia is severe, it is not compatible with survival.
Other Rare Anatomical Obstructions of the Airway
Sometimes a newborn has tumors or masses in the mouth, nasal cavity, neck, larynx, or trachea. These may significantly compress the airway and mediastinal structures. Tumors and masses can be detected clinically or with the use of radiologic imaging modalities.
The success of PPV via a face mask, endotracheal tube, or laryngeal mask depends on the location of the mass or tumor. If intubation or ET tube ventilation fails, then PPV via a laryngeal mask may suffice.
A specialist consult with a pediatric head and neck surgeon should be considered. Early detection prompts the obstetrician to deliver the baby at an institution specializing in the care of these patients.
17 Choanal atresia: unilateral. SickKids website. Accessed and image retrieved March 26, 2021.