Stroke: Assessment in the Emergency Department
This guide bridges the gap between prehospital emergency medical services (EMS) and in-hospital stroke care. Designed for paramedics, EMTs, and emergency department (ED) nurses, this article explains how to conduct a rapid prehospital stroke assessment, what critical information to report during handoff, and the exact 10-minute stabilization protocol patients undergo upon arriving at a stroke center.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- EMS transports stroke victims to hospitals with a Stroke Team whenever possible.
- A stroke victim’s general assessment in the ED should take no longer than 10 minutes.
- The NIH Stroke Scale and the Canadian Neurological Scale are stroke scales used for neurological assessment.
- The CT scan is the most important tool to distinguish between ischemic and hemorrhagic stroke.
- Stroke treatment involves fibrinolytic therapy for ischemic stroke and surgery for hemorrhagic stroke.
The EMS to ED Connection: The successful treatment of an acute stroke relies heavily on the prehospital assessment. Emergency medical service (EMS) providers are the first link in the chain of survival. Their primary goal is the accurate identification of stroke symptoms, stabilizing vital functions, establishing the critical “Time Zero” (the last time the patient was seen at their baseline normal), and providing pre-arrival notification to the receiving hospital so the ED can prepare.
Because time is brain tissue, EMS providers must choose health care facilities designated as stroke centers. Some hospitals aren’t equipped or experienced to handle acute stroke victims. If an acute stroke victim is taken to an under-equipped hospital, the facility must have a rapid protocol in place for immediate patient transfer to a suitable institution.1
Hospitals with stroke units have highly detailed provider roles to care for these patients. Neurology specialists decide on a definitive treatment strategy (e.g., fibrinolytic therapy to dissolve clots or endovascular therapy to mechanically remove them). Admitting a patient to a dedicated stroke unit significantly increases their survival rate, functional outcomes, and overall clinical outcome.
General Assessment
The initial evaluation and medical stroke assessment of a suspected patient is a rapid, collaborative effort. To ensure no time is wasted, it is important to distinguish which tasks happen in the field versus in hospital settings.
Prehospital (EMS) Actions:
- ABCs: Ensure Airway, Breathing, and Circulation are stable.
- Oxygen: Administer supplemental oxygen if O2 saturation is below 94%.
- Glucose Monitoring: Check a rapid fingerstick blood glucose to rule out hypoglycemia, which can mimic a stroke.
- Prehospital Neurologic Assessment: Perform a rapid screening using a standardized tool stroke (stroke screening tools like the FAST exam are most common).
- IV Access (If time permits): Establish intravenous access en route, but do not delay transport.
When calling the receiving ED, EMS should provide a concise “Stroke Alert” report: “We are en route with a [Age/Gender] presenting with right-sided weakness and aphasia. The Last Known Normal time is [Exact Time]. Blood glucose is 105. Vital signs are stable. ETA is 5 minutes.”
In-Hospital (ED) Actions:
When the patient arrives, emergency department personnel have a strict 10-minute window to perform their initial assessment, guided by protocols such as the adult suspected stroke algorithm.
- Activate the Stroke Team: The ED immediately pages the specialized Stroke Team (neurologists and specialized nurses) based on the EMS pre-arrival report.
- Blood Sampling: Draw comprehensive labs including a Complete Blood Count (CBC), electrolytes, and coagulation factors (to check how fast the blood clots) at a minimum.
- In-Hospital Neurologic Assessment: Perform a detailed exam using the National Institutes of Health Stroke Scale (NIHSS). For a step-by-step guide on how to do a neurological assessment, providers can reference standardized protocols to ensure accuracy.
- Order a CT Scan: The patient must be rushed to imaging for a non-contrast CT scan of the brain.
- 12-Lead ECG: Providers may perform an ECG to determine if an arrhythmia (like atrial fibrillation) or an acute myocardial infarction caused an embolic (clot-based) stroke.
To see how these critical steps come together in a clinical setting, watch this overview on What is Involved in General Stroke Care.
Neurologic Assessment
The neurological assessment differs significantly depending on whether the patient is still in the field with EMS or has arrived at the hospital.
Prehospital Stroke Screening
EMS providers use rapid screening tools to quickly identify stroke probability. The most common is the FAST exam (Face drooping, Arm weakness, Speech difficulty, Time to call). However, modern EMS protocols increasingly use advanced scales to screen for severe Large Vessel Occlusion (LVO). Whether isolated to a single large vessel or involving complex multi-vessel occlusion, these severe occlusion strokes require rapid transport to specialized comprehensive stroke centers. Common LVO-suspicion screens include:
- RACE (Rapid Arterial oCclusion Evaluation)
- FAST-ED (Field Assessment Stroke Triage for Emergency Destination)
- LAPSS (Los Angeles Prehospital Stroke Screen)
Watch Out for Stroke Mimics: EMS must remain vigilant for conditions that perfectly mimic stroke symptoms. Hypoglycemia (low blood sugar), post-seizure Todd’s paralysis, and complex migraines can all present with unilateral weakness and speech issues. Additionally, posterior circulation strokes (affecting the back of the brain) often present vaguely with intense dizziness, ataxia (loss of coordination), and vision changes, making them easy to miss if relying solely on basic FAST exams.
In-Hospital Stroke Scales
Once the patient arrives, the Stroke Team performs a highly detailed neurological assessment. They typically use the NIH Stroke Scale (NIHSS), a 15-item rating scale and neurological examination used to quantify the impairment and specific neurological deficit caused by a stroke, or the Canadian Neurological Scale (CNS), a slightly simpler scoring system evaluating consciousness, orientation, and motor function. (Later in the patient’s recovery, providers may also use the modified ranking scale to measure long-term disability)
The most critical part of this assessment is accurately determining the time of symptom onset. Providers must confirm the “Last Known Normal” time from multiple informants, asking bystanders or family exactly when they last perceived the patient to be normal. The complete in-hospital neurologic assessment should not exceed 25 minutes from the patient’s arrival at the door.

The NIH Stroke Scale is a primary tool for quantifying stroke severity in the ED.
Read: Immediate Ischemic Stroke Therapies
CT Scan: Ischemic versus Hemorrhagic Stroke

A non-contrast CT scan is required to differentiate between an ischemic clot and a hemorrhagic bleed.
Because the therapies for a clot are fatal if given to a patient with a brain bleed, treatment cannot begin until providers perform a non-contrast CT scan of the head.3 This imaging determines whether the patient is experiencing an ischemic stroke (blockage) or a hemorrhagic stroke (bleeding from a ruptured vessel or aneurysm).
Crucial Rule: Providers must absolutely withhold all fibrinolytic and anticoagulation medications (like tPA, aspirin, or heparin) until the CT scan conclusively rules out a hemorrhagic stroke. If the institution lacks a CT scan machine, they must stabilize the patient and immediately transfer them to an equipped hospital.
Time is critical: CT scan images must be completed within 25 minutes of patient arrival in the ED, and an expert radiologist should interpret them within 45 minutes. While advanced imaging like CT perfusion, CT angiography, or brain MRI can provide deeper diagnostic insight, ordering them should never delay the administration of fibrinolytic treatments if the patient is already a candidate.

CT scan for ischemic stroke (left) and hemorrhagic stroke (right).
Ischemic Route
If the CT scan confirms the stroke is due to ischemia and strictly rules out any intracerebral hemorrhage, the patient is immediately assessed for fibrinolytic therapy eligibility. If the patient meets the appropriate time window and medical criteria, a clot-busting drug like rTPA (recombinant tissue plasminogen activator) may be administered according to protocol. For a deeper review of fibrinolytic and endovascular options, see ischemic stroke treatment: immediate therapies. If the patient is not a candidate for fibrinolytics, providers will typically shift to antiplatelet therapy or other stroke-care pathways as appropriate. If the patient can’t swallow, an aspirin suppository is used.4

Hemorrhagic Route
If the CT scan confirms the stroke is hemorrhagic, a neurosurgeon must be consulted immediately. Fibrinolytics are strictly contraindicated. Providers must prepare the patient for rapid admission to a dedicated stroke unit or ICU, and initiate preparations for potential surgical intervention to stop the bleeding and relieve cranial pressure.
For a comprehensive breakdown of the pharmacological and surgical interventions used on these distinct pathways, review our lesson on the Immediate Therapies for Stroke.
Summary
Successful acute stroke care requires a seamless handoff between prehospital and in-hospital teams. EMS must rapidly screen the patient, pinpoint the exact “Last Known Normal” time, and provide pre-arrival notification to a designated stroke center. Upon arrival, the ED has exactly 10 minutes to stabilize the patient’s ABCs, draw labs, and activate the specialized Stroke Team. Finally, because therapies for clots are lethal for bleeds, no definitive treatment can begin until a rapid non-contrast CT scan differentiates an ischemic stroke from a hemorrhagic stroke.
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
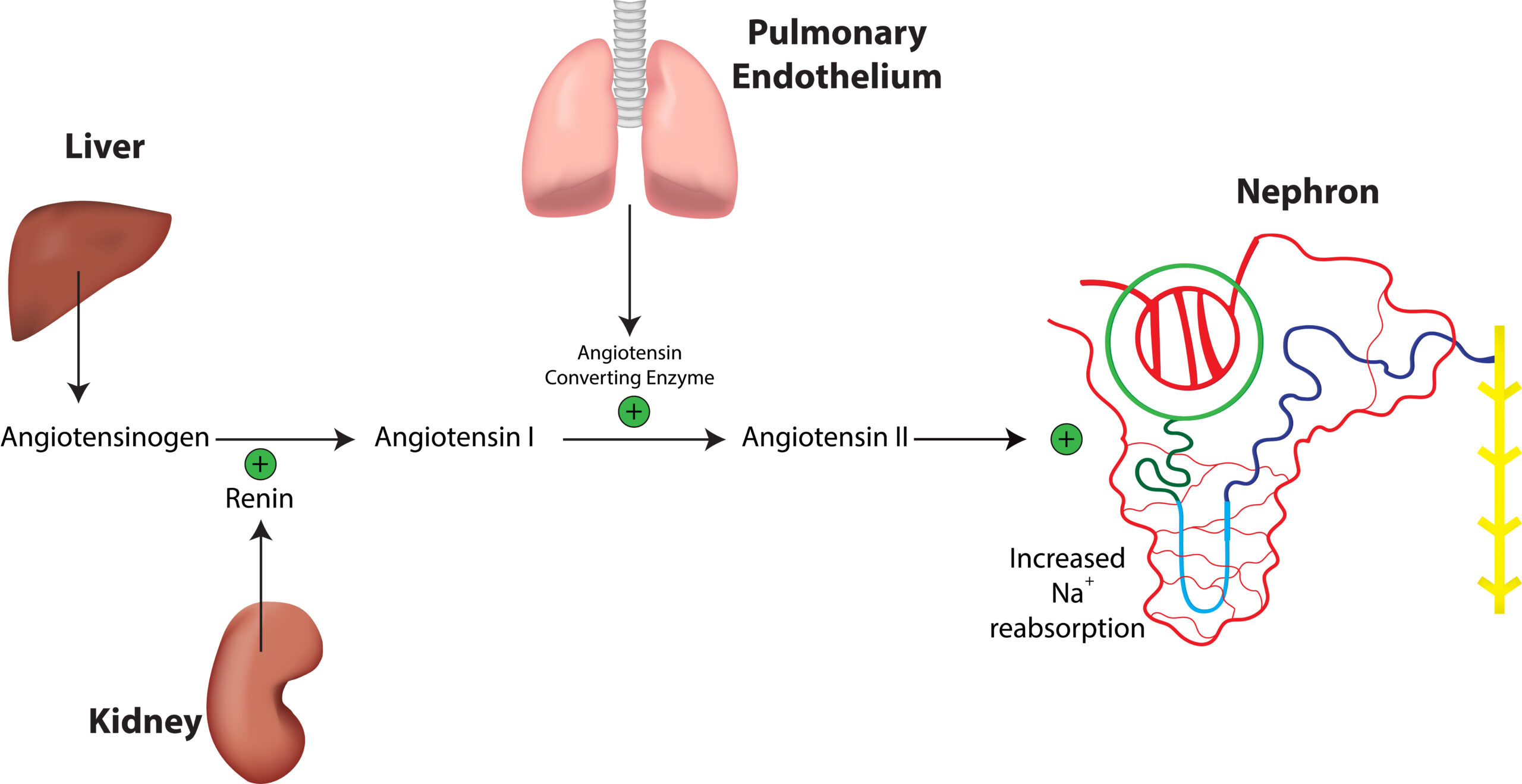
This article and video detail the Renin-Angiotensin-Aldosterone System (RAAS). Learn the pathophysiology of RAAS and drug...
This article and video explain the differences between DKA and HHS. Learn how hyperosmolar hyperglycemic syndrome differs from diabetic ketoacidosis.