SVT ECG Criteria (Supraventricular Tachycardia)
This guide is designed for healthcare professionals, ACLS providers, and medical students aiming to refine their rhythm interpretation skills. After reading, you will be able to confidently identify Supraventricular Tachycardia (SVT) on an ECG, distinguish it from common rhythm mimics, and understand the underlying criteria for accurate clinical diagnosis.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
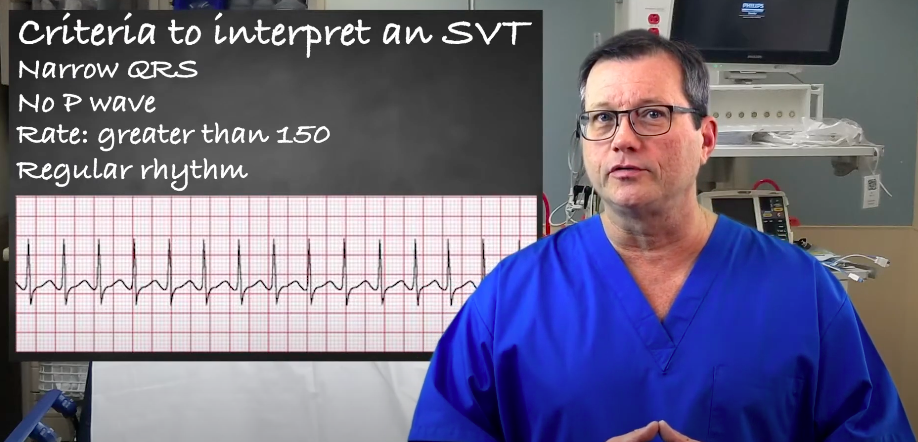
- Rate: Typically greater than 150 bpm.
- Rhythm: Regular.
- QRS Complex: Usually narrow (< 0.12 seconds).
- P Waves: Often hidden, absent, or retrograde due to the rapid rate.
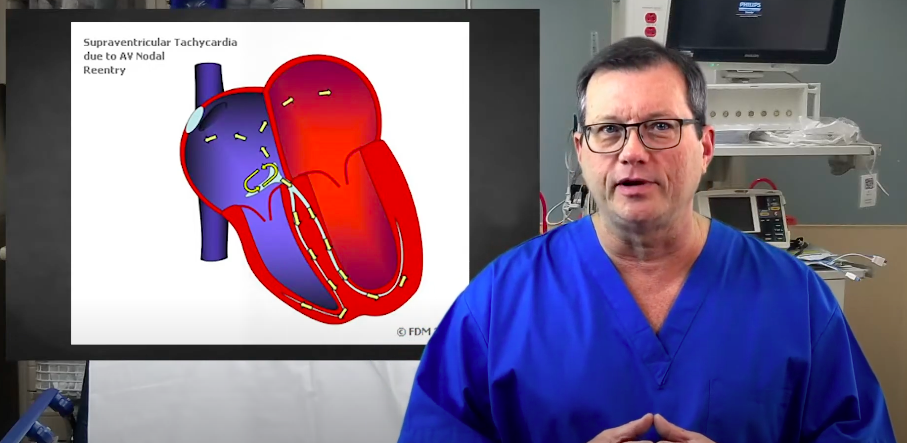
To interpret an SVT, remember the “S” stands for supra, connoting the complex’s origin above the ventricles. Most SVTs occur from a re-entry circuit somewhere around the AV node, and management should follow the ACLS tachycardia algorithm for appropriate intervention. Re-entry circuits cause SVTs, leading to hidden P waves and a fast ventricular rate. These re-entry circuits tend to be very quick. The overall ventricular rate for an SVT is typically greater than 150 bpm, frequently sitting between 150 and 250 bpm. There is usually only one re-entry pathway used at a time, meaning the R-R intervals should be identical and march out in a highly regular rhythm. Because the impulse originates above the ventricles and travels down the normal His-Purkinje system, it typically produces a narrow QRS complex (< 0.12 seconds). Since the complex originates around the AV node and the rate is so fast, normal P waves are not produced. P waves may be entirely absent, buried inside the QRS complex, or seen as a retrograde (inverted) wave just after the QRS. ECG Example: Notice the highly regular R-R intervals, narrow QRS complexes, and absent P waves characteristic of SVT. Criteria for SVT Interpretation Summary While SVT is classically a narrow-complex tachycardia, it can present with a wide QRS complex if the patient has a pre-existing Bundle Branch Block (BBB), rate-related aberrancy, or an accessory pathway (e.g., WPW syndrome). Wide-complex SVT can be diagnostically ambiguous and closely mimics Ventricular Tachycardia (VT). When in doubt, ACLS guidelines dictate treating undifferentiated wide-complex tachycardia as VT. Accurate diagnosis requires ruling out SVT mimics: Comparison: Differentiating SVT from Sinus Tachycardia, AFib, and Atrial Flutter relies on rate, regularity, and P-wave morphology. Read: Rhythm-based Management in Cardiac ArrestInterpreting a Supraventricular Tachycardia (SVT)
Step-by-Step ECG Interpretation Workflow
1. Rate
2. Rhythm Regularity
3. QRS Width Assessment
4. P Wave Assessment
The Wide-Complex Caveat
Differential Considerations: Common Pitfalls and Look-Alikes
Summary
Physicians and ACLS providers must know the specific criteria for Supraventricular Tachycardia to effectively guide treatment. Patients will typically exhibit a narrow QRS complex, an absent or hidden P wave, a heart rate greater than 150 bpm, and a highly regular rhythm. However, careful differentiation is crucial: always be aware of edge cases like atrial flutter with a 2:1 block, rapid atrial fibrillation, sinus tachycardia, or an SVT presenting with a wide QRS complex due to aberrancy.
To strengthen your foundational knowledge, review our ECG and Cardio Cycle Basics. For your next steps, continue practicing with real-world ECG strips and algorithms to master these subtle rhythm differences.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
Endotracheal Intubation is a method of placing a tube into the windpipe (trachea). The process opens an airway and help the patient who can't breathe on their own.
Download the Acute Coronary Syndrome: Managing NSTEMI PDF and view the videos to learn the treatment guidelines of managing NSTEMI.