Endotracheal Intubation: Advanced Airway Basics for ACLS and CPR
This comprehensive guide covers the essential principles of endotracheal intubation during resuscitation. Designed for ACLS providers, EMS professionals, and resuscitation teams, this article explores the indications for advanced airways, required equipment, pre-hospital decision-making, and how to verify tube placement using waveform capnography. What it is: Endotracheal intubation is a critical, life-saving procedure used to secure a patient’s airway, deliver oxygen, and prevent aspiration during severe illness or cardiac arrest.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Understand the exact indications and contraindications for placing an endotracheal tube during CPR.
- Learn how to systematically prepare equipment and optimize oxygenation prior to intubation attempts.
- Master the steps for verifying and monitoring tube placement using continuous waveform capnography.
- Endotracheal (ET) intubation requires specialized knowledge, practice, and experience to master.
- Endotracheal intubation should be performed during cardiopulmonary resuscitation (CPR) when other forms of airway management are insufficient or when CPR efforts are prolonged.
- Endotracheal intubation in the field requires expert knowledge and the ability to determine when to intubate and when to transport the patient as quickly as possible to the emergency department (ED).
- Everyone who assists with intubation should know how to intubate and the equipment needed.
- End-tidal CO2 monitoring can help to improve the quality of CPR.
Endotracheal intubation is the definitive method for securing an airway. As an advanced airway, it is frequently used in patients requiring prolonged CPR to protect the airway and prevent aspiration. Advanced airways use specialized equipment and require specific education and clinical experience to insert properly and safely.
They may be inserted “blindly” or by using a laryngoscope, an instrument consisting of a handle and a blade with a lighted end to visualize the vocal cords. There are several types of advanced airways with varying degrees of intrusiveness. While basic adjuncts (like oropharyngeal and nasopharyngeal airways) and supraglottic devices (tubes that sit above the vocal cords, like an LMA) have been covered previously, this article will focus exclusively on endotracheal intubation.

An endotracheal tube is a flexible plastic tube placed through the mouth (orotracheal) or nose (nasotracheal) into the trachea. The procedure of placing this tube is called intubation, which establishes a secure route to the lungs to assist with breathing and protect against aspiration.
Endotracheal Intubation
Endotracheal intubation is a dynamic procedure that requires careful preparation and strict adherence to protocols. This section breaks down the clinical indications, field decision-making for paramedics, required equipment, and strict confirmation steps.
General Intubation Workflow:
- Assess: Determine if the patient meets the indications for an advanced airway.
- Prepare: Gather and test all intubation and backup equipment.
- Pre-oxygenate: Optimize the patient’s oxygen saturation.
- Intubate: Visualize the cords and pass the tube.
- Confirm & Secure: Verify placement with waveform capnography and secure the tube.
Indications and Contraindications
Endotracheal intubation is indicated in several critical scenarios:
- Airway Protection: When it is necessary to control and protect the patient’s airway from aspiration.
- Gas Exchange Failure: When gas exchange is deranged and intubation will enable clinicians to correct hypoxia, acidosis, or alkalosis through mechanical ventilation.
- Prolonged CPR: When resuscitation efforts are extended and an unprotected airway poses risks.
- Long-term Maintenance: When the patient requires airway maintenance for long periods.
Intubation is generally contraindicated when patients have conditions that can be corrected in a short time without invasive airway management. From a practical standpoint, note that intubation is not always necessary immediately during CPR if adequate ventilations are being provided with a bag-mask device. However, prolonged use of a bag-mask device increases the risk of insufflation of the stomach and subsequent regurgitation, which is why an advanced airway is eventually considered.
Most medical providers have heard the saying: “Just because you can, doesn’t mean you should.” [cite: 815] Intubation is not without risks, such as interrupting chest compressions or causing airway trauma. Paramedics should keep that in mind before performing endotracheal intubation in the field. [cite: 816] Field Decision Framework: Paramedics should ask themselves the following questions to determine if they should intubate now or use an alternative and transport: Answering these questions will help paramedics in the field make the important determination of whether to intubate. For example, if a patient is 3 minutes from a trauma center and can be adequately ventilated with a bag-mask, delaying transport to attempt a difficult intubation in the field is not ideal; prioritize transport. If transport is 30 minutes away, establishing a definitive airway becomes a higher priority. Other points to consider include: Early consultation with the ED physician at the receiving hospital can help paramedics make difficult intubation decisions. Read: Stroke: Assessment and Important Time Frames Outside of the HospitalEndotracheal Intubation in the Pre-hospital Setting
Equipment Needed
It is important to know the equipment intimately and be ready for intubation at a moment’s notice, whether in the field or in the ED. Necessary equipment includes the following organized categories:
Preparation & Pre-oxygenation:
- Yankauer suction tip catheter and suction tubing (must be set up and turned on before intubating).
- Resuscitation bag (bag-mask device) attached to 100% oxygen (set up before intubating).
Intubation Tools:
- Laryngoscope handles and blades: curved (MacIntosh) and straight (Miller) blades of various sizes; ensure the light is functioning.
- Cuffed endotracheal tubes of different sizes (average size for an adult is 7.5).
- Stylet (a malleable wire placed inside the ET tube to give it shape).
- Syringe (to inflate the cuff on the ET tube).
- Lubricating jelly (water soluble).
Backup & Advanced Tools:
- Oral and nasal airways of various sizes.
- Bougie tube (a flexible introducer used when vocal cords are difficult to visualize).
- McGill forceps (specialized tongs used to guide the tube or remove foreign bodies).
Confirmation & Securing:
- Carbon dioxide monitoring device (waveform capnography).
- Commercial tube securing device or tape.

Equipment needed for intubation includes the laryngoscope, endotracheal tube, and a resuscitation bag.
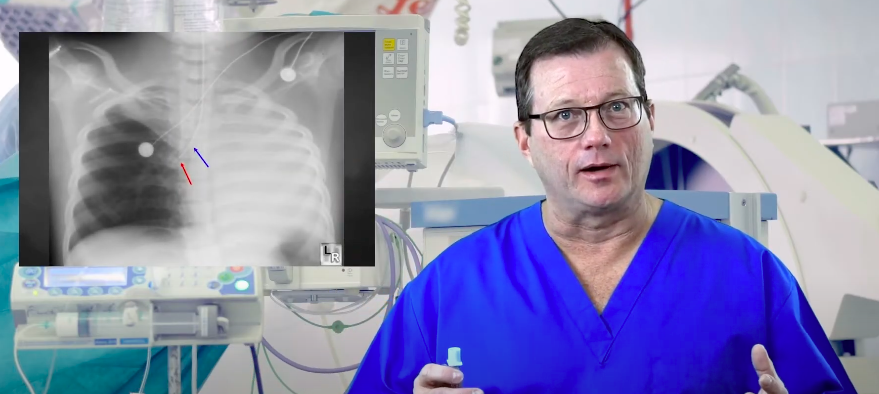
It is critical to confirm placement to avoid pushing the tube too deep. If inserted too far, the tube typically enters the right lung, leaving the left lung unventilated. Review our guide on ET tube depth for practical tips on correct positioning. Learn How Do You Correct a Right Mainstem Intubation in this brief video lesson.
Preparation and Intubation Procedure
In the hospital setting, the equipment above is often kept in a kit or in a drawer of the crash cart for easy access. Equipment should be checked frequently for expiration dates and to ensure that no equipment is missing. All team members must know where to find all equipment when needed and should understand how to set it up and prepare for use.
Specialized equipment, such as fiberoptic scopes and difficult intubation kits, may also be available in the hospital setting.
In cases of cardiac arrest, sedating the patient prior to intubation is not necessary. However, in most other instances, sedation is required prior to intubation. Sedation relaxes the muscles and facilitates easier intubation, and it makes the patient more comfortable. Generally, a paralytic agent is given, along with a muscle relaxant and pain medication.
Prior to intubation, it is important to ensure that the patient’s oxygenation status is optimized. This does NOT mean that the patient should be hyperventilated. To optimize oxygenation, provide free flow oxygen from the resuscitation bag or provide high flow oxygen with a nasal cannula. A nonrebreather mask can also be used to hyperoxygenate the patient prior to intubation.

The intubation procedure is performed to control and protect the patient’s airways.
Once the patient has been successfully intubated by the most experienced team member, it is important to secure the airway to prevent dislodgement of the tube. That can be achieved using tape or a commercial device. Providers should always document the tube’s position (e.g., “22 cm at the teeth”) and reassess and re-secure the tube any time the patient is moved or transported.
Confirmation Checklist:
Tube placement must be confirmed immediately to ensure oxygen is reaching the lungs and not the stomach.
- Primary Confirmation: Ensure there is a CO2 detector attached to the ET tube (preferably continuous waveform capnography) to verify tracheal placement.
- Auscultation & Chest Rise: Listen for bilateral breath sounds and observe bilateral chest wall rise. Ensure there are no gastric sounds.
- Monitor for Complications: Clinicians must be alert for complications such as a right mainstem intubation, which can cause unilateral breath sounds and inadequate ventilation.
- Secondary Confirmation: An X-ray can confirm tube depth placement, but the X-ray must wait if the patient is in active cardiac arrest.
If an intubated patient suddenly deteriorates, providers must quickly identify the cause. Learn the standard mnemonic for troubleshooting advanced airways in our D.O.P.E. for Intubated Patients video lesson.
Waveform Capnography
Waveform capnography is a method of measuring end-tidal carbon dioxide (EtCO2) levels — the amount of carbon dioxide that is produced after the exhalation phase of respiration. [cite: 864] It can be measured if the patient has an advanced airway in place, such as an endotracheal tube.
As seen in the visual patterns above, the presence of carbon dioxide after exhalation creates a distinct waveform. This indicates that there is gas exchange within the alveoli; [cite: 865] it also indicates adequate pulmonary blood flow.
During cardiac arrest, end-tidal carbon dioxide levels closely reflect the cardiac output that is generated by chest compressions. [cite: 866] The normal end-tidal carbon dioxide measurement is 35–45 mm Hg in adults with a spontaneous pulse. [cite: 867] However, during CPR, it is recommended that end-tidal carbon dioxide levels be maintained between 10–20 mm Hg. The 10-20 mm Hg range indicates that CPR quality is optimal and that the chances of return of spontaneous circulation (ROSC) are also good. [cite: 868]
What to do if EtCO2 is low (< 10 mm Hg) during CPR:
- Assess compressor fatigue and switch compressors.
- Ensure compression depth is at least 2 inches (5 cm).
- Ensure the compression rate is between 100-120 per minute.
- Allow for full chest recoil between compressions.
Waveform capnography can also inform resuscitation decisions. A poor prognosis may be considered if, after 20 minutes of high-quality CPR, waveform capnography consistently records less than 10 mm Hg of carbon dioxide.
In summary, there are many uses for quantitative waveform capnography:
- It measures the quality of CPR. [cite: 869]
- It can help prognosticate the outcome of the resuscitation effort. [cite: 870]
- It validates proper endotracheal tube placement. [cite: 871]
- It validates cardiac output and pulmonary perfusion. [cite: 872]
- It can guide mechanical ventilation settings. [cite: 873]
What is the difference between endotracheal intubation and a tracheostomy?
Endotracheal intubation is a temporary, acute measure where a tube is passed through the mouth or nose and down into the trachea. A tracheostomy is a surgical procedure where an incision is made directly into the front of the neck (trachea) to place a breathing tube, typically used for long-term airway management when a patient cannot be safely extubated.
Summary
Endotracheal intubation is the definitive airway management strategy for patients in respiratory failure or cardiac arrest. While advanced airways provide optimal ventilation and protect against aspiration, their placement requires specialized equipment and trained providers. It is important that the medical team is practiced in inserting endotracheal tubes and has the necessary equipment at hand. [cite: 874] Furthermore, once an endotracheal tube is placed, continuous waveform capnography is essential—not only to confirm initial tracheal placement, but to actively monitor the effectiveness of CPR chest compressions throughout the resuscitation effort.
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
1. Christopher Newell, Scott Grier, and Jasmeet Soar. Airway and ventilation management during cardiopulmonary resuscitation and after successful resuscitation. Critical Care. 2018.
2. Joshua T. Bucher; Rishik Vashisht; Megan Ladd; Jeffrey S. Cooper. Bag Mask Ventilation. National Library of Medicine. 2022.
3. David M. Gnugnoli; Abhishek Singh; Katherine Shafer. EMS Field Intubation. National Library of Medicine. 2022.
4. Andres L. Mora Carpio; Jorge I. Mora. Ventilator Management. National Library of Medicine. 2022.
5. Richardson M, Moulton K, Rabb D. Capnography for Monitoring End-Tidal CO2 in Hospital and Pre-hospital Settings: A Health Technology Assessment. CADTH Health Technology Assessment, No. 142.2016.
6. Bhavani Shankar Kodali and Richard D. Urman. Capnography during cardiopulmonary resuscitation: Current evidence and future directions. Journal of Emergencies, Trauma, and Shock. 2014.
2.
More to Learn
Learn how to correct right mainstem intubation and achieve the target range for endotracheal (ET) tube placement. Our article helps enhance patient safety and airway management.
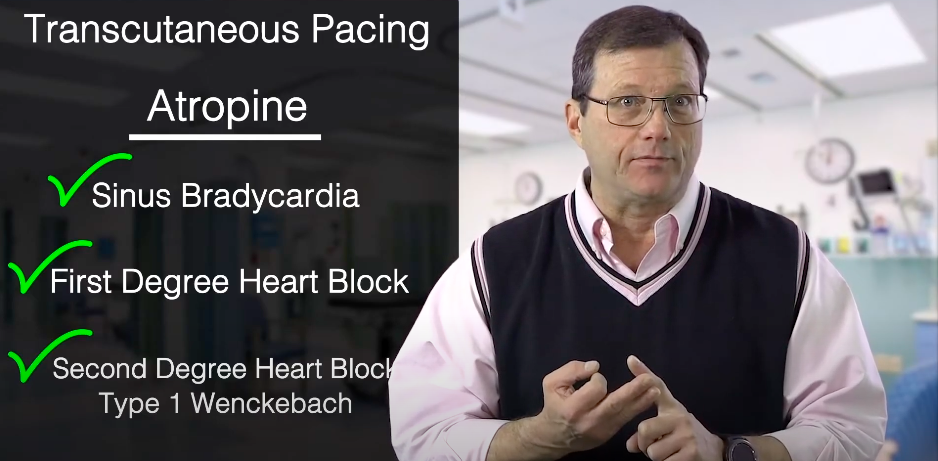
Discover transcutaneous pacing, pad placement, and cardiac monitors at ACLS Certification Association. Our article enhances your knowledge of life-saving interventions.