Criteria for PACs (Premature Atrial Contractions)
This guide is designed for healthcare professionals, nursing students, and ACLS providers aiming to master the identification of Premature Atrial Contractions (PACs). By the end of this article, you will understand the specific ECG criteria, common causes, and how to quickly differentiate a PAC from other arrhythmias to ensure an accurate diagnosis and improve the overall patient outcome.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Atrial fibrillation is characterized by:
- Regularity: Very irregular
- Rate: Atrial rate > 350 bpm but difficult to measure; ventricular rate < 100 bpm
- P Wave: Unable to discern
- PR Interval: Not measurable
- QRS Complex: < 0.12 seconds
- What is a PAC? A single, early electrical impulse originating in the atria.
- Key ECG Feature: An early P wave with an altered shape, usually followed by a normal, narrow QRS complex.
- Not AFib: While PACs originate in the atria, they are isolated early beats, not Atrial Fibrillation (AFib), which is a completely chaotic and sustained rhythm.
Premature Atrial Contractions
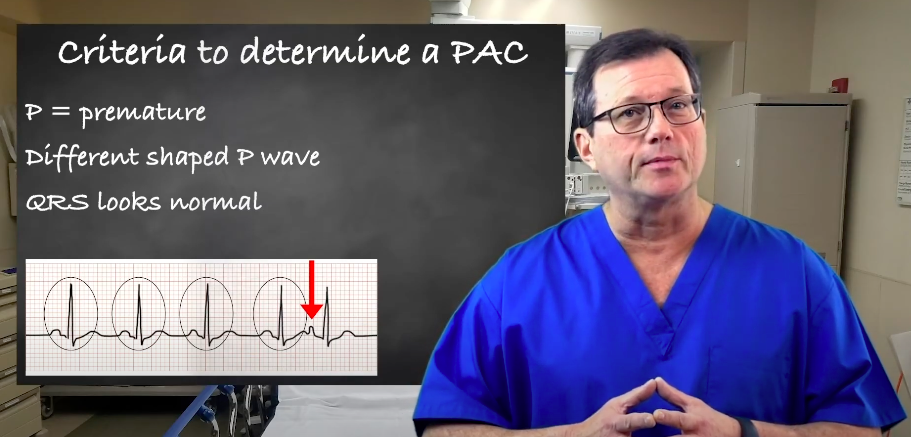
A Premature Atrial Contraction (PAC) is an early, ectopic electrical signal that originates in the atrial tissue, outside of the normal sinoatrial (SA) node. The “P” in PAC stands for premature, meaning the complex occurs prior to the next expected beat in the underlying rhythm. As the R waves march out on the ECG tracing, the PAC disrupts the regularity.
![]()
The red arrow points to a complex that has occurred prior to the next expected beat.
The “A” stands for atrial. Because this impulse originates from a different area of the atria, it takes a different pathway, creating a differently-shaped P wave. The P wave is typically upright, but its morphology will vary from a normal sinus P wave. In some cases, it may be flattened, peaked, or even buried in the preceding T wave, making it difficult to spot.
The P wave is upright but looks different.
The QRS complex interval is usually narrow (less than 0.12 seconds) because the impulse typically follows the normal ventricular conduction pathway. However, exceptions do occur, such as a PAC with aberrant conduction, which can result in a temporary wide QRS complex. Generally, the QRS interval should match the other normal QRS complexes on the strip.
The three determinants for a PAC
PAC ECG Criteria Checklist:
- Timing: The beat is premature (early).
- P Wave: Present, but the shape (morphology) differs from the underlying sinus P waves.
- QRS Complex: Usually narrow, matching the underlying rhythm.
Common Symptoms of PAC
Many patients are completely asymptomatic. When symptoms do occur, they typically include:
- A feeling of a “skipped” heartbeat.
- Palpitations or a brief fluttering sensation in the chest.
- Mild anxiety associated with the irregular beat.
Common Triggers and Contributors of PAC
PACs are incredibly common in healthy individuals, but their frequency can be increased by:
- High caffeine or alcohol intake.
- Stress, anxiety, and fatigue.
- Electrolyte imbalances (e.g., low potassium or magnesium).
- Underlying heart disease (such as heart failure) or hypertension, which can increase the overall risk of frequent PACs.
What’s the difference between premature atrial contractions and premature ventricular contractions?
The key difference lies in where the ectopic beat originates:
- PACs originate in the atria. They have an abnormal P wave followed by a narrow QRS.
- PVCs (Premature Ventricular Contractions) originate in the ventricles. They have NO preceding P wave and feature a wide, bizarre QRS complex.
- PJCs (Premature Junctional Contractions) originate in the AV junction. They have a narrow QRS, but the P wave is usually absent or inverted.
Are premature atrial contractions the same as atrial fibrillation?
No. A PAC is a single, early heartbeat that interrupts an otherwise normal underlying rhythm. Atrial Fibrillation (AFib) is a sustained, chaotic rhythm where the atria quiver instead of contracting effectively. While frequent PACs can sometimes be a precursor to AFib, they are distinct conditions.
How to Identify a PAC on ECG (Step-by-Step)
When interpreting a rhythm strip, follow these steps to reliably identify a PAC rather than calculating a sustained rate like 60-100 beats per minute (bpm).
- Assess Timing: Look at the R-R intervals. Find the spot where the rhythm suddenly becomes irregular because a beat arrived too early.
- Compare P Waves: Look immediately to the left of the early QRS. Is there a P wave? If yes, compare its shape to the P waves of the normal beats. If it looks different, it’s a PAC.
- Match QRS Width: Ensure the QRS complex of the early beat is narrow and matches the morphology of the normal beats around it.
To see these steps applied in real-time, watch this ECG Rhythm Review for PAC, which highlights how the premature complex alters the typical cardiac cycle.
Summary
A PAC comes prematurely, so the P wave occurs before the next expected complex on the ECG strip. The P wave’s morphology will differ. It will still be upright but a little flattened. The QRS complex remains the same as PAC doesn’t impact ventricular conduction. In metabolic emergencies, clinicians often compare conditions like HHS vs DKA to differentiate causes of instability.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
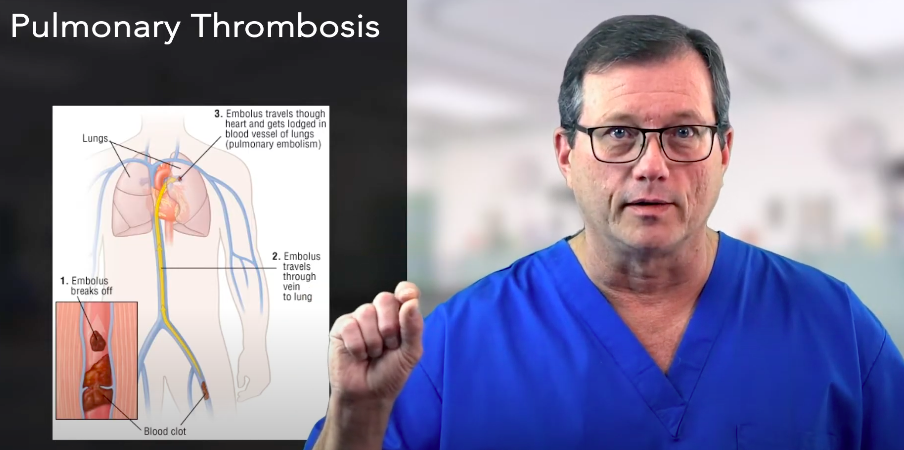
Discover Hs and Ts lessons for pulmonary embolism in our article. Gain insights into identifying and managing potentially reversible causes for improved patient outcomes.
When the patient is stable and the tachyarrhythmia persists, determine if the QRS-complex is narrow or wide for the correct treatment of the patient. Read more in our detailed article.