Fixing Right Mainstem Intubation
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- After intubation, the provider must know how to correct a right mainstem intubation.
- The provider uses sight and sound to determine how far to withdraw the tube.
- The provider listens on the left side and slowly withdraws the ETT until breath sounds are heard
Basic Intubation Overview and How Over Advancement Happens
Endotracheal tubes are placed to deliver ventilation directly into the trachea so both lungs can be ventilated. After the tube passes the vocal cords, it is secured at a measured depth at the teeth or gums and then reassessed. Even when the tube is correctly placed at first, it can move deeper with patient movement, transport, or when the head and neck position changes.
Over advancement happens when the tube tip migrates beyond the carina and enters a mainstem bronchus. This produces endobronchial intubation, which typically ventilates only one lung. For a full walk through of technique and monitoring, review endotracheal intubation and waveform capnography concepts.
This short overview reinforces correct tube placement steps, how to confirm position, and how to avoid common airway complications. Watch the video for a clear overview before focusing on correcting the right mainstem.
You may have to correct a right mainstem intubation in a case where, hypothetically, an overzealous rescuer buried the endotracheal (ET) tube, and it went into the right lung, highlighting the importance of proper airway management. The doctor may look at the X-ray and ask you to pull it back two centimeters. While you could simply move it two centimeters, you could also use sight and sound to help guide the ET into a better position. This X-ray image shows a right mainstem intubation. First, look at the size of the ET tube at the hub to get a target range of where you want to be at the patient’s teeth. Next, while someone else bags the patient, take the cuff down, deflate the cuff, and listen to the left side of the chest with a stethoscope as you retract the tube. As you pull the ET tube back, make sure to look at the ET tube markings, ensuring you don’t go past the target range. Pull the tube back until you hear lung sounds, for quick tooth‑to‑carina rules of thumb and expected centimeter ranges by patient size, see ET tube depth. It’s much better to use sight and sound to position the ET tube opposed to randomly pulling it back two centimeters which may possibly extubate the patient. Read: General Stroke Care Pay attention to the target range of the ET tube. Listen to the left lung while pulling the ET tube back. This video explains how clinicians estimate and confirm appropriate endotracheal tube depth and why depth matters for preventing mainstem placement. Check out the video below to refresh your depth planning skills and reassess after making a move.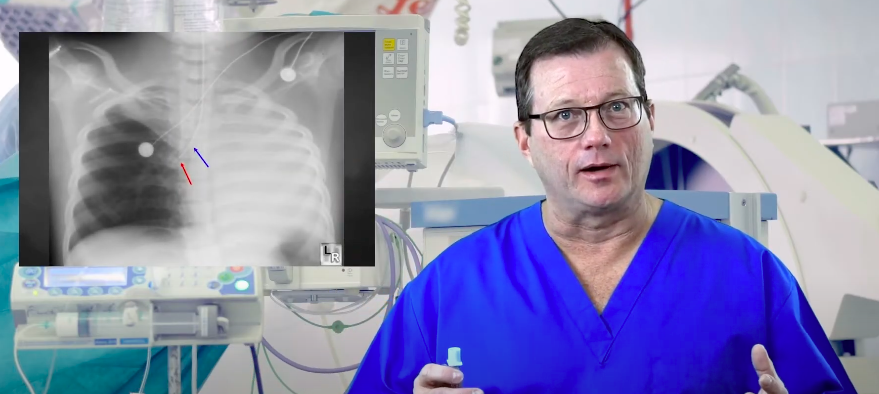
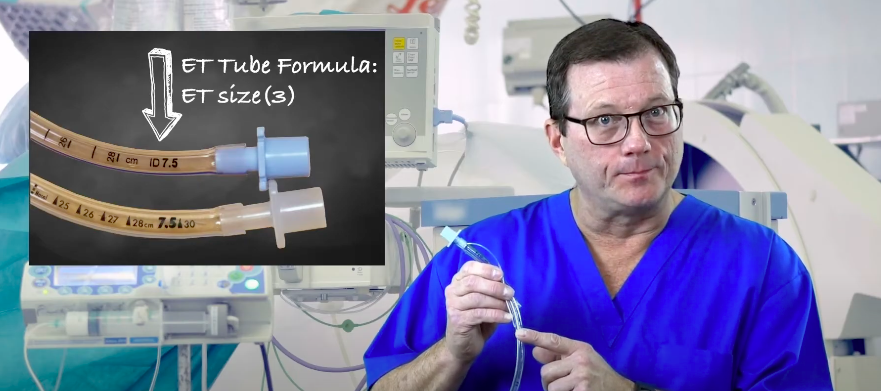
How Do You Calculate Tube Depth?
Right mainstem intubation is more common because the right main bronchus is typically wider and more vertical than the left. The left main bronchus angles more sharply as it travels toward the left lung. When an endotracheal tube is advanced too far, the tip naturally follows the path of least resistance and can enter the right main bronchus. Practical takeaway: if a patient becomes harder to ventilate after tube placement, or breath sounds drop on the left, consider right mainstem placement early and confirm quickly.Anatomical Factors: Why the Right Mainstem is More Common
Diagnostic Indicators: Identifying Endobronchial Placement
Clinical Signs (Sight & Sound)
- Asymmetrical chest rise: right side rises more than left
- Breath sounds: decreased or absent breath sounds on the left when auscultating
- Ventilation feel: increased resistance during bagging, higher peak pressures on a ventilator
- Oxygenation change: falling SpO2 or worsening color despite ongoing ventilation
Clinical exam is fast and should be repeated after any movement, transport, or repositioning. Use the stethoscope on both sides and reassess tube depth markings at the teeth.
Technical Confirmation
- Waveform capnography: confirms tracheal placement but does not confirm depth, so use it alongside exam
- Tube depth markings: compare the centimeter marking at the teeth to expected depth for the patient
- Chest x ray: can show the tube tip position relative to the carina and is commonly used for confirmation
- Ultrasound: may support assessment of lung sliding and ventilation symmetry when available
Key point: end tidal CO2 confirms you are in the airway, but depth problems still require clinical assessment and imaging when available.
Complications of Uncorrected Endobronchial Intubation
If a mainstem intubation is not corrected, only one lung receives most of the ventilation. This can cause inadequate oxygenation and ventilation, and it can also injure the ventilated lung due to overinflation.
- Hypoxemia: reduced oxygenation because the non-ventilated lung is not participating
- Atelectasis: collapse of the under-ventilated lung, commonly the left
- Barotrauma: overdistention of the ventilated lung, increasing risk of pneumothorax
- Worsening hemodynamics: hypoxia and high intrathoracic pressures can affect circulation
- Delayed recognition: outcomes worsen when the problem is discovered late during transport or after position changes
Corrective Maneuver: Repositioning and Depth Optimization
If right mainstem placement is suspected or confirmed, correction is usually a controlled withdrawal of the tube to the appropriate depth while reassessing ventilation. Use a systematic approach so you do not accidentally extubate the patient.
- Stabilize and call out the plan: ensure someone is ventilating the patient and monitoring oxygenation while you adjust the tube.
- Confirm the current depth: read the centimeter marking at the teeth or gums and note the current position.
- Prepare to reposition: if recommended by your protocol, reduce cuff pressure or briefly deflate the cuff so the tube can be withdrawn smoothly.
- Withdraw slowly in small increments: pull back a small amount while watching the depth markings and staying within a safe target range.
- Reassess with sight and sound: check for improved symmetrical chest rise and listen for return of left sided breath sounds during ventilation.
- Reinflate and secure: reinflate the cuff as appropriate, secure the tube firmly, and document the final depth marking.
- Reconfirm position: reassess waveform capnography, repeat auscultation bilaterally, and obtain imaging confirmation when available.
Practical tip: Using depth markings plus lung sounds is more reliable than blindly pulling the tube back a fixed number of centimeters, because patient anatomy and initial depth vary.
Right mainstem intubation occurs when the endotracheal tube is advanced past the carina and ventilates one lung, most often the right. Recognize it early using clinical signs like unequal chest rise and decreased left breath sounds, then confirm with depth markings and imaging when available. Correct it with a controlled withdrawal, reassessing lung sounds and ventilation symmetry while tracking the centimeter mark at the teeth. After repositioning, secure the tube and reconfirm ventilation using repeat exam, waveform capnography, and follow-up confirmation as appropriate.Summary
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
Learn Managing Respiratory Arrest and Maintaining Airway Patency, including Oropharyngeal and Nasopharyngeal Airway Management in our detailed article and video illustrations.

Download the PDF for the Adult Bradycardia with a Pulse Algorithm that explains the step-by-step process of assessing and treating patients with symptomatic bradycardia.