How to Interpret Arterial Blood Gases
An arterial blood gas (ABG) is a blood sample taken from an artery. It measures oxygenation, ventilation, and acid-base balance, helping you identify respiratory versus metabolic problems and whether compensation is occurring. This lesson reviews how to interpret an arterial blood gas by examining the different ABG components. Then, we’ll use an easy method to systematically go through the numbers to accurately interpret the ABG to provide better treatment.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Table of Contents
- Arterial Blood Gases Introduction
- Components of an Arterial Blood Gas
- PaO2 (pO2): What it means on an ABG
- pCO2
- HCO3 (Bicarbonate)
- pH: How to tell acidemia vs alkalemia
- Interpreting the ABG
- Step 1: Start with the pH
- Step 2: Look at the pCO2
- Step 3: Look at the bicarbonate
- Compensation
- Mixed Blood Gas
- Summary
Article at a Glance
- Arterial blood gas (ABG) interpretation includes a review of pH, PCO2, HCO3, and PO2.
- The PO2 normal range is 80-100 and indicates the body’s ability to take up oxygen.
- pH indicates the amount of acid in the body, with a lower pH indicating a higher acid level. Normal = 7.35-7/45.
- PCO2 is a respiratory acid with a normal range between 35-45. If the number increases, the result is respiratory acidosis, and if it decreases, it is respiratory alkalosis.
- HCO3, or bicarbonate, is a metabolic base with a normal range of 22-26. If the number increases, metabolic alkalosis develops.
- Compensation occurs when the respiratory or metabolic system attempts to return the pH to normal.
This lesson reviews how to interpret the results from arterial blood gas tests. The article will examine the different ABG components. Then, we’ll use an easy method to systematically go through the numbers to accurately interpret the ABG to provide better treatment.Arterial Blood Gases Introduction
Related Video – Understanding and Interpreting ABGs Part 1: Introduction to ABGs
Components of an Arterial Blood Gas
What is measured in an arterial blood gas test?
An ABG test provides several values, which can be divided into core interpretation values and other standard measurements:
- Core Acid-Base Values: pH, PaCO2 (carbon dioxide), and HCO3- (bicarbonate).
- Oxygenation Values: PaO2 (oxygen partial pressure) and SaO2 (oxygen saturation).
The primary components of an ABG are the pH, pCO2, HCO3–(bicarbonate), and pO2. We’ll start with pO2, since we don’t use it to interpret acid-base status on an ABG. But it’s still important, so let’s review.
The four key components of an arterial blood gas are pH, pCO2, HCO3- (bicarbonate), and pO2.
PaO2 (pO2): What it means on an ABG
pO2, also notated as paO2, stands for the partial pressure of oxygen in the arterial bloodstream. The pO2 notates the body’s ability to take up oxygen. A normal pO2 level is between 80 and 100 mmHg. Interestingly, the pO2 on a blood gas should be about five times the FiO2, or the fraction of inspired oxygen, the patient is receiving.

When a patient on oxygen has a return of spontaneous circulation, we need to throttle back on the FiO2 to prevent oxygen toxicity.
Room air hovers around 21% oxygen. A normal pO2 on room air is 21 times 5, which gives us around 80 to 100 mmHg. If you’re administering 100% oxygen to your patient, your predicted pO2 is 100 times 5, or about 500 mmHg. If, after administering that dose, the pO2 on the patient’s blood gas is only 200, something is off. For some reason, the patient can’t take up the oxygen.
For ACLS, we’ve discovered both oxygen toxicity and free radicals are damaging during a return of spontaneous circulation (ROSC). One study suggests a pO2 greater than 350 mmHg after ROSC was associated with poor outcomes. So, once we get a pulse and circulation back, we have to start throttling back the FiO2 to achieve a normal pO2 on a blood gas.
pCO2
pCO2, also expressed as paCO2, stands for the partial pressure of CO2 in the arterial bloodstream. Remember, for the purposes of ABG interpretation, the pCO2 is a respiratory acid.
A normal pCO2 level is between 35 and 45 mmHg. If a patient accumulates this respiratory acid, their pCO2 number goes up, and they will develop respiratory acidosis. If the number drops below 35, they’ll develop a respiratory alkalosis.
Related Video – Understanding and Interpreting ABGs Part 4: Respiratory Alkalosis
Related Video – Understanding and Interpreting ABGs Part 5: Respiratory Acidosis
Exhaling helps to get rid of CO2, a respiratory acid.
The body controls the pCO2 level through ventilation.
First, oxygen comes into the cell. The cell uses the oxygen and the byproduct is pCO2. pCO2 is like the exhaust of the cells. If you’re breathing normally, your pCO2 is going to be fine. If you’re not breathing enough, a common complication for patients with a severe pulmonary disease, the exhaust builds up leading to respiratory acidosis, which highlights the importance of a thorough respiratory assessment.
If you breathe too fast, you’ll exhaust your pCO2, and its level in your body will drop. The pH balance swings the other way, resulting in respiratory alkalosis.
Read: ACLS Drugs – Lidocaine
HCO3 (Bicarbonate)
HCO3–, or bicarbonate, is a metabolic base. Metabolic base refers to an alkaline, or an antacid. A normal bicarbonate level is 22–26 mmol/L. If a patient’s metabolic base increases, their bicarbonate level is elevated, resulting in a metabolic alkalosis. If the bicarbonate level drops below 22 mmol/L, the patient may develop metabolic acidosis.
Related Video – Understanding and Interpreting ABGs Part 7: Metabolic Acidosis
pH: How to tell acidemia vs alkalemia
Usually the more of something you have, the greater the numeric value. Remember, pH operates differently than other substances, as the pH number actually drops in accordance with increased hydrogen levels. Keep that in mind to avoid mistakes when interpreting an ABG. Thus, when pH drops, a patient becomes acidotic.
A decreasing pH means it is becoming more acidic, while an increasing pH signifies it is becoming more basic.
Interpreting the ABG
Related Video – Easy Interpretation of Arterial Blood Gases
To interpret an ABG, first decide if the pH is acidotic or alkalotic. Next, check PaCO2 for a respiratory cause, then check HCO3 for a metabolic cause. Finally, decide whether compensation is present or if a mixed disorder is likely. There are several steps involved in reading a blood gas, but remember to always start with the pH.
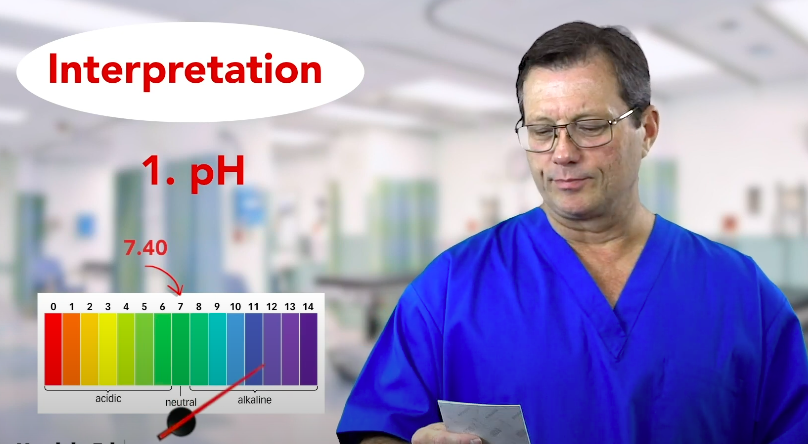
Step 1: Start with the pH
A normal pH is between 7.35 and 7.45. A “perfect” pH would be 7.40. If it’s not normal, first determine whether it’s more acidic or alkaline.
If a pH blood gas is 7.3, remember that pH can only “fall” into acid. If the pH numbers have fallen, the pH reflects an overall acidosis. Next, find what’s contributing to the acidosis. Check the pCO2 and bicarbonate because they offer information about the acid-base status. Check if either reflects in acidosis.
Step 2: Look at the pCO2
Next, look at the pCO2, or respiratory acid. In this case, the pCO2 is 30 mmHg. The pCO2 level is lower than the normal range of 35–45 mmHg, so that represents a respiratory alkalosis. It might seem odd to have an acidic pH but a respiratory alkalosis. So we must look at our other measurements to find the acidosis.
Step 3: Look at the bicarbonate
The bicarbonate measurement is 20. We know that bicarbonate is a metabolic base, and the normal bicarbonate level is between 22 and 26. The decreased level of bicarbonate reflects a metabolic acidosis.
Compensation
Compensation happens when the respiratory or metabolic system shifts in the opposite direction to bring pH toward normal. If the pH is still abnormal, compensation is partial. If the pH returns to the 7.35 – 7.45 range, compensation is full. One side compensates for the other by attempting to blow off or retain acid to correct the internal balance of acids and bases.
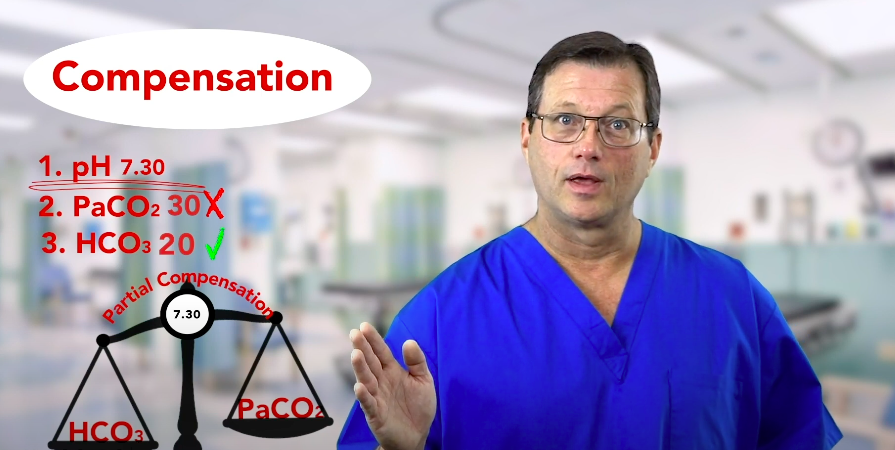
In partial compensation, the compensation does not return the pH to a normal level. In full compensation, the pH returns to a normal level.
Remember, compensation means either the respiratory or metabolic component has moved outside of its normal range in the opposite direction to compensate for the other side.
For example, your patient has a pH reflecting acidosis. Their pCO2 is normal, so the respiratory component is normal. Next, you notice the bicarbonate, or the metabolic component, reflects a metabolic acidosis. The respiratory component did not compensate. We know this because the pCO2 stayed within its normal range. If the pCO2 had compensated, it would have been a respiratory alkalosis.
Overall, compensation works three ways:
- No compensation: the metabolic or the respiratory component stayed within normal range and did not compensate for the other side.
- Partial compensation: there is compensation, but it did not return the pH to normal range.
- Full compensation: The compensation returns the pH to normal range.
Mixed Blood Gas
Patients can exhibit a mixed blood gas, meaning a metabolic and respiratory acidosis or metabolic and respiratory alkalosis. These particular patients are very sick and require immediate expert consultation.
Summary
The components of an ABG are the pH, pCO2, HCO3–(bicarbonate), and pO2. All four of these measurements have standard ranges. If the patient’s blood gases fall outside of the standard range, they may experience respiratory/metabolic acidosis or alkalosis. Respiratory compensation occurs when the body attempts to correct, for instance, a metabolic acidosis via a compensatory respiratory alkalosis. There may be no compensation, partial compensation, or full compensation.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn

This article and video reviews Beta Blockers vs. Beta Agonists. Understand how Beta Blockers are used in treatment for cardiovascular...
Our article interprets several criteria on a patient’s ECG tracing to determine atrial fibrillation. Gain insights into identifying and diagnosing this common cardiac arrhythmia.