Premature Junctional Contractions (PJC): ECG Criteria, Causes & Symptoms
Premature junctional contractions (PJC) are early beats that originate near the AV node instead of the SA node. On ECG, a PJC often shows an inverted P wave before the QRS, an inverted P wave after the QRS, or no visible P wave because it is hidden in the QRS. In this guide, you will learn the most common causes, typical symptoms, and step by step ECG criteria so you can identify PJC confidently on a rhythm strip.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- PJCs are characterized by:
- Regularity: PJC interrupts the underlying rhythm
- Rate: Depends on the rate of the underlying rhythm
- P Wave: P wave preceding the PJC may be before or after QRS or hidden within the QRS
- PR Interval: Normal in underlying sinus rhythm, typically < 0.20 seconds if inverted P wave precedes the QRS; otherwise, no measurable PRI
- QRS Complex: Typically < 0.12 seconds and appears before the next expected beat
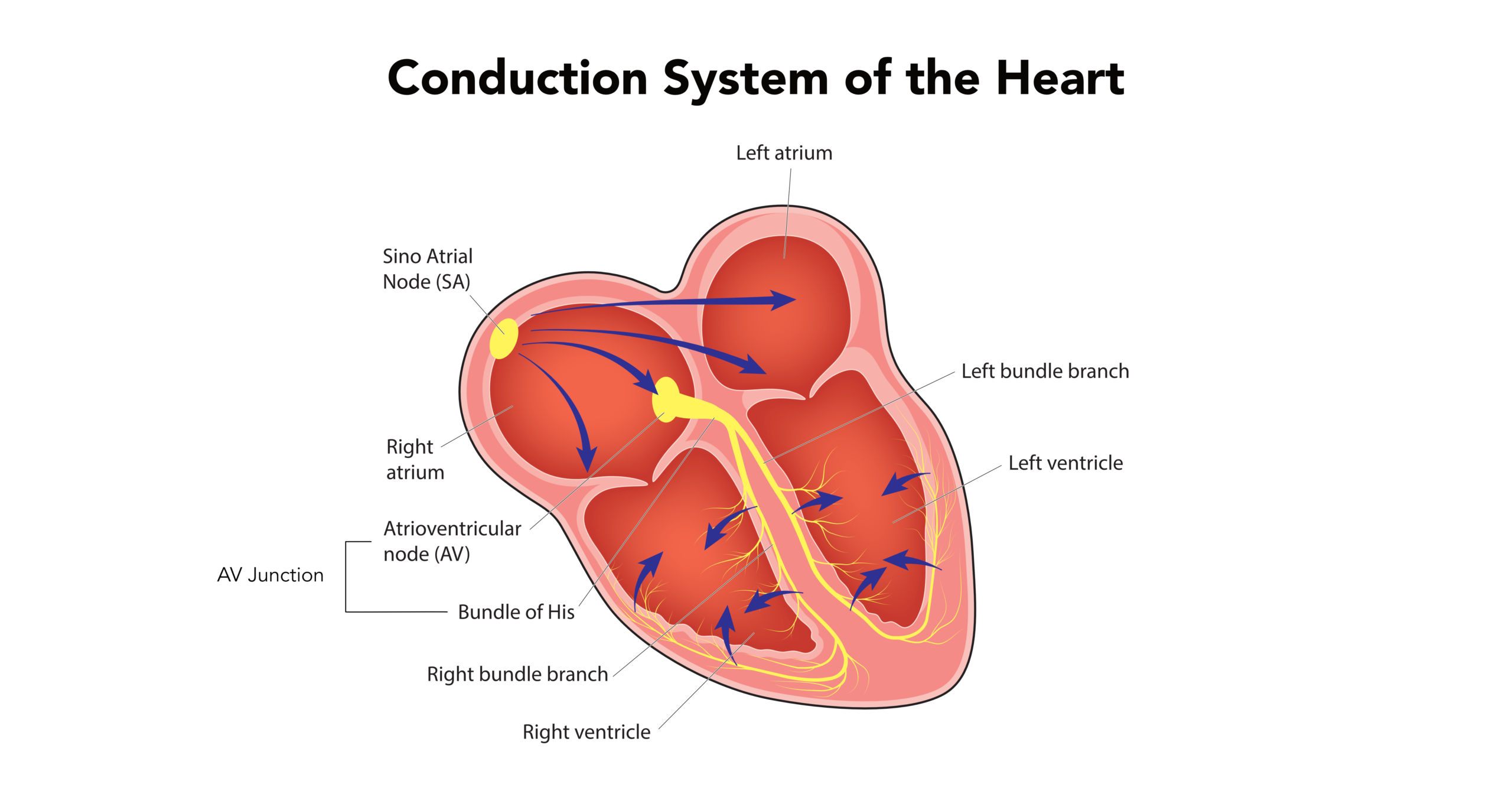
A PJC (also known as a junctional extrasystole) is a premature beat that arises from the atrioventricular (AV) junction of the heart, presenting as a unique type of junctional rhythm. The “P” stands for premature, so this complex will appear prior to the next expected beat. As the R-waves march out, this complex comes before the next expected complex. If you want a quick refresher on how electrical conduction creates the waves and intervals on an ECG, this short lesson is the best starting point. It helps you connect P waves, PR interval timing, and QRS appearance before you evaluate ectopic beats. The premature junctional contraction (PJC) is marked with a red arrow. The “J” connotes that the beat comes from the junction. The heart’s junction is where the atria and ventricles meet. When the junction fires off, it sends a wave of electricity, retrograde, back through the atria, creating an inverted P wave. You’ll either have an inverted P wave before the QRS complex, no P wave at all, or an inverted P wave after the QRS complex. Read: Criteria for PACs (Premature Atrial Contractions) During PJC, the conduction starts at the AV node and then moves in both directions simultaneously down through the ventricles and retrograde through the atrial chambers. In a PJC, the conduction starts at the AV node as opposed to the sinoatrial (SA) node. The PJC should have no impact on ventricular conduction, so the QRS complex should appear normal. This walkthrough shows a real rhythm strip and highlights the premature timing, the P wave relationship, and the narrow QRS that points to a junctional origin.Premature Junctional Contractions
ECG and the Cardiac Cycle Basics
![]()

ECG Strip: Premature Junctional Complex (PJC)
Common Causes of PJCs and Cardiac Triggers
PJCs can appear in healthy individuals, especially when the body is under stress or stimulated. They can also occur in patients with underlying cardiac conditions. In many cases, identifying and removing triggers is enough to reduce how often they happen.
- Stress and increased adrenaline: anxiety, pain, fever, dehydration, and poor sleep
- Stimulants: caffeine, nicotine, energy drinks, and some decongestants
- Electrolyte imbalance: low potassium or low magnesium can increase ectopy
- Hypoxia: reduced oxygen from respiratory illness can increase irritability
- Medication effects: some medications may affect automaticity or conduction in sensitive patients
- Cardiac causes: ischemia, cardiomyopathy, structural heart disease, or post procedure irritation
Clinical note: If PJCs suddenly increase in frequency, check for reversible triggers first, especially stimulants, dehydration, hypoxia, and electrolyte issues.
Identifying Symptoms of Premature Junctional Complexes
Many people with occasional PJCs feel nothing. When symptoms happen, they are usually caused by the sensation of an early beat and the pause that sometimes follows.
- Palpitations, fluttering, or a skipped beat feeling
- A brief thump sensation in the chest
- Lightheadedness, especially if PJCs are frequent
- Fatigue or mild shortness of breath in sensitive individuals
Seek urgent evaluation if symptoms include fainting, persistent chest pain, significant shortness of breath, or signs of poor perfusion.
ECG Criteria for Premature Junctional Contractions
Use this checklist to identify a premature junctional contraction on a rhythm strip. The goal is to confirm that the beat is early, junctional in origin, and conducted normally through the ventricles.
- Establish the underlying rhythm. Identify the baseline rhythm and estimate the expected timing of the next beat.
- Find the premature beat. A PJC appears earlier than the next expected complex and interrupts the regular pattern.
- Evaluate the P wave. Look closely around the premature QRS:
- Inverted P wave before the QRS, often with a short PR interval
- No visible P wave because it is buried in the QRS
- Inverted P wave after the QRS due to retrograde atrial activation
- Measure the QRS duration. In most PJCs, the presentation is a narrow QRS complex that is typically under 0.12 seconds.
- Check for a pause. A brief pause can occur, but it is often not a fully compensatory pause like you would see with a PVC.
- Compare with PAC and PVC. Use the differential table below when the strip is unclear.
Practical tip: A narrow premature QRS with an inverted or missing P wave strongly supports PJC, especially when the P wave timing is before, within, or after the QRS.
PJC vs. PAC vs. PVC: How to Tell the Difference
When the ECG strip is fast or noisy, these three findings help separate atrial, junctional, and ventricular ectopy.
| Feature | PAC | PJC | PVC |
|---|---|---|---|
| P wave shape | Usually present, often different from normal sinus P | Inverted before QRS, inverted after QRS, or absent | Usually absent before QRS, may have retrograde P after |
| PR interval duration | Usually measurable, may be normal or slightly different | Often short if inverted P precedes QRS, otherwise not measurable | Usually not measurable before QRS |
| QRS complex width | Narrow, typically under 0.12 seconds | Narrow, typically under 0.12 seconds | Wide, typically 0.12 seconds or greater |
Shortcut: Wide premature QRS strongly suggests PVC. Narrow premature QRS suggests PAC or PJC, then P wave inversion and timing often points to a PJC (a junctional ectopic beat).
Clinical Significance and Management of Junctional Ectopy
Occasional PJCs are often benign, especially in patients with no structural heart disease and no concerning symptoms. When they are frequent or symptomatic, management focuses on stability, triggers, and targeted evaluation.
- Assess symptoms and stability: check vitals, perfusion, chest discomfort, shortness of breath, and mental status
- Look for triggers: caffeine, nicotine, dehydration, fever, hypoxia, and recent medication changes
- Correct reversible causes: fluids when appropriate, treat fever, improve oxygenation, correct electrolytes based on clinical judgment
- Consider monitoring: if frequent, new, or symptomatic, ambulatory monitoring may help quantify ectopy burden
- Escalate when needed: syncope, persistent chest pain, hemodynamic instability, or suspected ischemia requires urgent evaluation
Documentation tip: record the premature timing, P wave relationship, QRS width, and patient symptoms to support a clear rhythm interpretation.
Summary
A premature junctional contraction arises from the heart’s AV junction. During a PJC, providers will observe either an inverted P wave before or after the QRS complex or no P wave at all. The QRS complex should be normal.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
The junctional rhythms include junctional tachycardia, accelerated junctional, and the junctional escape rhythm.
Uncover the potential of Adenosine Injection in ACLS drug therapy for SVT. Our article details proper dosing and administration for effective life-saving interventions.