Atrioventricular Blocks
This comprehensive guide covers the identification, causes, and clinical management of atrioventricular blocks. Designed for ACLS providers, nurses, and medical students, this resource will enable you to confidently identify varying degrees of AV blocks on an ECG strip and determine the appropriate urgency and treatment pathways for your patients.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
Core Takeaway: Atrioventricular blocks represent a delay or complete failure of the electrical signals traveling from the atria to the ventricles, categorized by severity from first-degree (delayed) to third-degree (completely blocked).
- AV blocks represent varying degrees of impulse blockages from the atria to the ventricles.
- In a first-degree AV block, the PR interval is uniformly prolonged.
- A second-degree type 1 block presents an increasing PR interval until a QRS complex is dropped.
- In a second-degree type 2 AV block, P waves “march through” in a consistent manner.
- A third-degree block has a complete dissociation between the atria and ventricles. Each beats at an independent rate.
What is atrioventricular block?
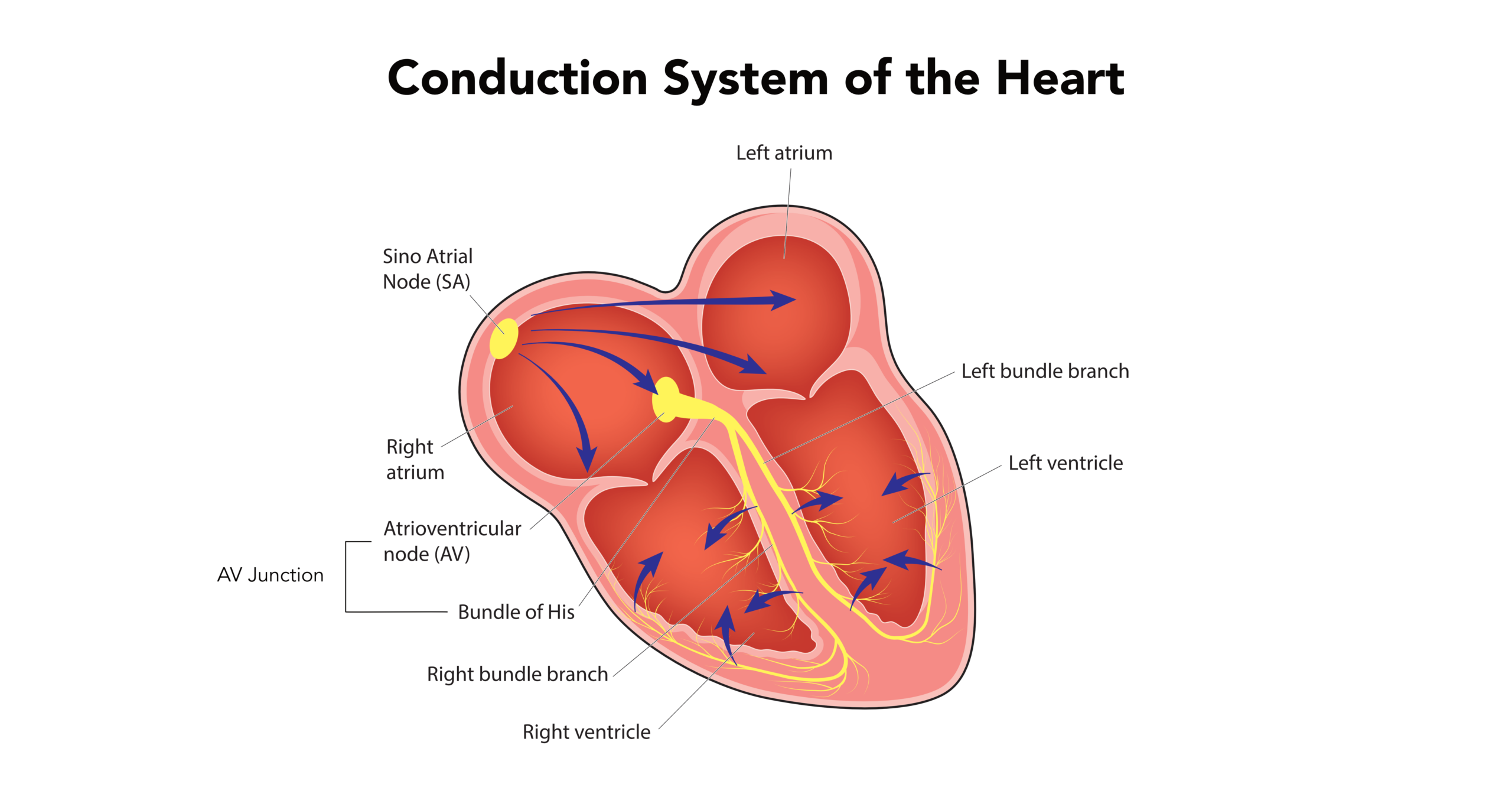
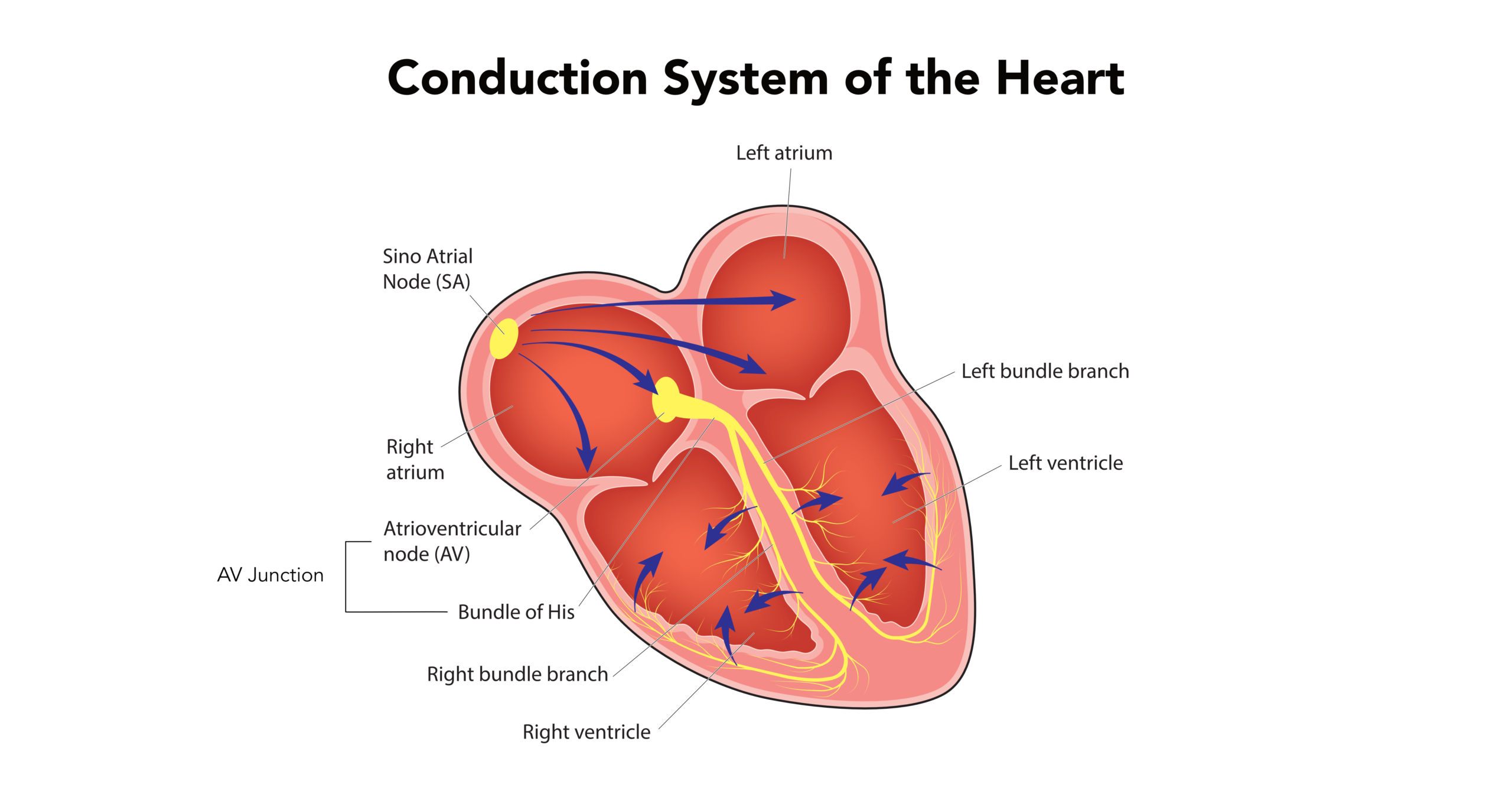
Atrioventricular blocks (AV blocks) are conduction delays that may cause a complete blockage of impulses from the atria to the ventricles. A heart block occurs when the electrical signal traveling through the heart is impaired, preventing the lower chambers from receiving the necessary pacing signals to contract effectively.
Atrioventricular blocks (AV blocks) are conduction delays that may cause a complete blockage of impulses from the atria to the ventricles.1 An increase in vagal tone during sleep, athletic training, pain, or stimulation of the carotid sinus may cause AV blocks.

What causes atrioventricular block?
AV blocks can stem from benign physiological responses to severe structural damage. Common causes include:
- Vagal Tone: An increase in vagal tone during sleep, athletic training, pain, or stimulation of the carotid sinus may cause AV blocks.
- Ischemic and Structural Disease: Ischemic heart disease causes 40% of AV blocks. Patients with cardiomyopathies, myocarditis, congenital heart disease, and familial disease may also develop AV blocks.
- Infiltrative/Inflammatory: Hereditary fibrosis or sclerosis of the cardiac skeleton, known as idiopathic progressive cardiac conduction disease (a gradual, unexplained degeneration of the conduction pathways) may damage the conduction system, causing AV blocks.
- Medications: Conduction-slowing medications such as verapamil, diltiazem, amiodarone, and adenosine can induce AV nodal blockade.
- Metabolic/Electrolyte: Separate from medications, raising the potassium concentration above 6.3 mEq/L (severe hyperkalemia) can drastically impair cardiac conduction.
- Iatrogenic: It may also be iatrogenic in nature (caused by medical examination or treatment), such as a catheter ablation in patients with arrhythmias.
What are the symptoms of atrioventricular block?
Symptom severity is directly linked to the degree of the block and the resulting heart rate. First-degree blocks and second-degree Mobitz Type 1 blocks are typically benign and asymptomatic, though some patients may report feeling “skipped beats.” Conversely, high-grade blocks (Mobitz Type 2 and Third-Degree) often cause severe hemodynamic instability due to profound bradycardia. These severe symptoms include dizziness, extreme fatigue, chest pain, shortness of breath, and syncope. Patients with a third-degree AV block may have ventricular standstill, leading to sudden cardiac death.
How is atrioventricular block diagnosed?
While rhythm strips are essential, diagnosing an AV block is a comprehensive clinical process. It begins with a 12-lead ECG to confirm the specific degree and location of the block. Providers must then conduct a thorough patient history and medication review to identify reversible pharmacological causes. Laboratory tests, such as a basic metabolic panel, are used to identify electrolyte imbalances such as hyperkalemia, while echocardiograms may be ordered to assess underlying structural heart disease.
How to identify AV block on an ECG (step-by-step)
To accurately classify an AV block, systematically evaluate the heart rhythm using this framework:
- Rate: Is the underlying atrial and ventricular rate normal or bradycardic?
- Rhythm: Is the rhythm regular, regularly irregular, or completely dissociated?
- P Waves: Is there a P wave for every QRS? Are they upright and uniform?
- PR Interval: Is the interval prolonged? Is it constant, or does it progressively lengthen?
- QRS Complex: Is it narrow (indicating AV node origin) or wide (indicating lower His-Purkinje origin)?
| Block Type | PR Interval Behavior | Dropped Beats? | P to QRS Relationship |
|---|---|---|---|
| 1st Degree | Consistently prolonged (>0.20s) | No | 1:1 (Always connected) |
| 2nd Degree (Mobitz I) | Progressively lengthens | Yes (Patterned) | Grouped beating |
| 2nd Degree (Mobitz II) | Constant (may be prolonged) | Yes (Intermittent) | Multiple P’s per QRS |
| 3rd Degree | Varies entirely | N/A (No conduction) | Completely dissociated |
First-Degree AV Block
Clinically, a first-degree atrioventricular block (often simply referred to as a first-degree atrioventricular delay) represents a delay, rather than a failure, in electrical conduction. If the PR interval is consistently prolonged (more than 0.20 seconds), it’s a first-degree AV block. Occasionally, you may see a “marked first-degree” block where the PR interval is excessively long (>0.30 seconds), causing the P wave to hide within the preceding T wave.
Structural defects within the atrioventricular (AV) node—the electrical relay station connecting the upper and lower chambers—or an increase in vagal tone due to conduction-slowing medications such as digoxin, beta-blockers, and calcium channel blockers cause first-degree AV block. Because no actual “block” (dropped beat) occurs, most cases are harmless and transient.

A P wave embedded within the T-wave and a PR-interval of about 0.28 seconds.
What are the First-Degree Heart Block Criteria?
This brief video highlights the essential ECG criteria for identifying a first-degree heart block, specifically focusing on how to measure a prolonged, constant PR interval. For an in-depth breakdown, visit our complete guide to First-Degree Heart Block criteria.
- RATE: depends on the core rhythm.
- RHYTHM: depends on the core rhythm.
- P WAVES: upright and uniform; each P wave is followed by a QRS complex.
- PR INTERVAL: more than 0.20 seconds, constant throughout the 6-second rhythm strip.
- QRS COMPLEX: less than 0.12 seconds.
Common Mistake: Failing to notice a prolonged PR interval when the heart rate is fast and the P wave becomes buried in the preceding T wave. Always measure carefully from the beginning of atrial depolarization to the start of the QRS.
Second-Degree (Mobitz Type 1) AV Block
A second-degree atrioventricular block has occasional non-conducted P waves with a prolongation of the PR interval. A second-degree atrioventricular Mobitz type 1 block (also known as Wenckebach) is an intermittent conduction block within the AV node, causing conduction impulse failure from the atria to the ventricles.
The impaired nodal conduction is progressive and results in a total block, causing an absence of impulse to the ventricles, as reflected in the QRS complex disappearing on the ECG tracing. There is a prolongation of the PR interval with each beat until a beat is dropped. This pattern repeats.

An ECG tracing of a second-degree Mobitz type 1 AV block.
The figure above shows a clustering of the first four QRS complexes. Clinicians should note the prolongation of the PR interval followed by the absence of a QRS complex. To see how these clustered patterns present dynamically, review this ECG Rhythm Review for Wenckebach blocks.
Mobitz type 1 AV block is generally benign. It rarely causes hemodynamic instability in patients, and most do not require any treatment. When a patient with Mobitz type 1 AV block has symptoms, they generally respond well to atropine. In rare cases, a pacemaker is required.
What are the Second-Degree (Mobitz Type 1) Heart Block Criteria?
The key to spotting Wenckebach is recognizing the progressive PR lengthening. Unlike Mobitz Type 2, which drops beats unpredictably, Mobitz Type 1 always exhibits a predictable “longer, longer, drop” pattern. This video clearly explains how to identify the criteria. For further reading, see our full guide on Second-Degree Type 1 criteria.
- RATE: may be bradycardia.
- RHYTHM: regularly irregular with a grouped beating pattern.
- P WAVES: upright and uniform; some P waves are not followed by a QRS complex.
- PR INTERVAL: progressively lengthens until one P wave is blocked and the QRS is dropped.
- QRS COMPLEX: less than 0.12 seconds.
Read: Junctional Rhythms
Related Video – ECG Rhythm Review – Second Degree Type 1 Heart Block (Wenckebach)
- RATE: may be bradycardia.
- RHYTHM: regularly irregular with a grouped beating pattern.
- P WAVES: upright and uniform; some P waves are not followed by a QRS complex.
- PR INTERVAL: progressively lengthens until one P wave is blocked and the QRS is dropped.
- QRS COMPLEX: less than 0.12 seconds.
Read: Junctional Rhythms
Second-Degree (Mobitz Type 2) AV Block
A second-degree Mobitz type 2 AV block involves the His-Purkinje system (the specialized fibers responsible for rapidly carrying electrical signals deep into the ventricles). A block occurs after the atrioventricular node, within the bundle of His or both bundle branches.
The His-Purkinje system is an all-or-none conduction system. Because of this, there are no progressive changes in the PR interval, even after a non-conducted P-wave. The P waves “march through” (appear at exactly regular intervals) at a constant rate. A Mobitz type-II AV-block carries a significantly higher risk of advancing to complete heart block compared to a Mobitz type I AV block.
This rhythm is considered a serious, potentially unstable arrhythmia. If left untreated, it may lead to severe bradycardia, profound hypoperfusion, and potentially death. Patients exhibiting this rhythm will often require temporary pacing and likely a permanent pacemaker.

An ECG tracing of a constant PR- and R-R interval until a dropped beat (QRS complex) occurs.
When interpreting the ECG tracing above, observing the constant PR interval is key. To practice differentiating this serious block from benign patterns, watch this ECG Rhythm Review for Second-Degree Heart Block (Type 2).
What are the Second-Degree (Mobitz Type 2) Heart Block Criteria?
Diagnostic Warning: Differentiating Mobitz I from Mobitz II can be difficult if there are not enough consecutive conducted beats to observe the PR interval behavior. If the PR behavior cannot be fully observed, rely on your step-by-step ECG framework and treat with caution.
- RATE: bradycardia; half to a third of patients have a normal rate.
- RHYTHM: R-R interval can be regular or irregular; P-P interval is regular.
- P WAVES: upright and uniform; more than one P wave for every QRS complex.
- PR INTERVAL: always constant across the strip; can be greater than 0.20 seconds.
- QRS COMPLEX: less than 0.12 seconds.
2:1 AV block and high-grade second-degree AV block
Sometimes a second-degree block presents with exactly two P waves for every one QRS complex (a 2:1 conduction ratio). Because there are never two consecutive conducted beats, it is impossible to see if the PR interval is lengthening (Mobitz I) or constant (Mobitz II). This is simply labeled a “2:1 AV Block.” High-grade second-degree AV blocks occur when two or more consecutive P waves are blocked (e.g., a 3:1 or 4:1 ratio), indicating profound conduction system disease that requires aggressive management.
Third-Degree AV Block
Third-degree AV block is a complete electrical dissociation between the upper and lower chambers (the atria ventricles). Impulses from the atria cannot reach the ventricles, so the perfusing rhythms are governed entirely by lower junctional or ventricular escape rhythms. Because these escape rhythms are slow and unreliable, this total AV dissociation creates profound hypoperfusion, which can rapidly deteriorate into ventricular standstill and sudden cardiac death. Patients with a third-degree AV block urgently need a pacemaker.
Third-degree AV block is secondary to atrioventricular nodal disease and involves the His-Purkinje system. Common contributing factors include:
- Coronary artery disease or acute myocardial infarction.
- Enhanced vagal tone or congenital disorders.
- Structural heart disease (hypertrophy, inflammation, or infiltration).
- Systemic conditions like Lyme disease, cardiomyopathies, autoimmune diseases, amyloidosis, sarcoidosis, or muscular dystrophy.
As mentioned, third-degree blocks force the heart to rely on lower escape rhythms. To understand how these lower pacemakers keep the patient alive, review our lesson on understanding Junctional Rhythms.

An ECG strip shows a third-degree AV block.
In the above strip, P waves occur every 0.92 seconds and the R-R interval is every 1.24 seconds, representing a dissociation in impulse rates from the atria and ventricles. Notice how the P waves “march” right through the QRS complexes. See this dissociation analyzed dynamically in our ECG Rhythm Review for Third-Degree Heart Block.
What are the Third-Degree Heart Block Criteria?
To confirm complete AV dissociation, check for these strict parameters. You can also explore our dedicated criteria breakdown for Third-Degree Complete Heart Block.
- RATE: atrial rate is 60–100 beats per minute (bpm); ventricular rate is 40–60 bpm if the focus is junctional or 20–40 bpm if the focus is ventricular.
- RHYTHM: regular.
- P WAVES: upright and uniform; more P waves than QRS complexes.
- PR INTERVAL: no relationship between P waves QRS complexes, and other features; P waves may occasionally be buried within the QRS complex.
- QRS COMPLEX: QRS complex is less than 0.12 seconds if the focus is junctional; 0.12 seconds or greater if the focus is ventricular.
How is atrioventricular block treated?
Treatment of an AV block is dictated by the degree of the block and the presence of hemodynamic instability.
- First-Degree: Generally requires no treatment. Monitor the patient and document the findings.
- Second-Degree (Mobitz I): Usually asymptomatic and benign. If symptoms arise, patients typically respond well to Atropine.
- Second-Degree (Mobitz II): Considered unstable. Do not rely on Atropine; prepare for temporary transcutaneous pacing. The patient will likely require a permanent pacemaker.
- Third-Degree: A medical emergency. Initiate transcutaneous pacing immediately and consult cardiology for permanent pacemaker implantation.
Reversible Causes and Medication Review
In all degrees of block, the clinical team must rapidly evaluate for reversible causes. Withdrawing AV nodal blocking medications (like beta-blockers or calcium channel blockers) or aggressively treating electrolyte imbalances (like severe hyperkalemia) can sometimes resolve the block entirely without surgical intervention.
Summary
AV blocks are caused by heightened degrees of impulse blockages from the atria to the ventricles. The different types of AV block include first-degree, second-degree type 1, second-degree type 2, and third-degree blocks. Each has its own diagnostic signature involving the relationship between the P wave and the QRS complex. While first-degree block is generally a benign delay requiring observation, untreated third-degree block presents a high risk of lethal ventricular standstill and demands immediate pacing.
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
1. Anthony H. Kashou; Amandeep Goyal; Tran Nguyen; Lovely Chhabra. Atrioventricular Block. National Library of Medicine. 2021.
2. Keri Wiginton. What Is Atrioventricular (AV) Block? WebMD. 2022.
3. Muhammad Asif Mangi; Wesley M. Jones; Mohamed K. Mansour; Laura Napier. Atrioventricular Block Second-Degree. National Library of Medicine. 2021.
4. Vinicius Knabben; Lovely Chhabra; Matthew Slane. Third-Degree Atrioventricular Block. National Library of Medicine. 2022.
More to Learn
In this course, learn about the rhythms that originate in the sinoatrial node, including normal sinus rhythm, sinus bradycardia, sinus tachycardia, and sinus arrhythmia.
The junctional rhythms include junctional tachycardia, accelerated junctional, and the junctional escape rhythm.