Electrolytes Explained
This video introduces the major electrolytes covered in this guide: sodium, potassium, calcium, magnesium, phosphorus, and chloride. After watching, learners should be able to connect electrolyte values with fluid balance, nerve signaling, muscle contraction, cardiac rhythm, and acid-base balance.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Electrolytes are charged minerals that help regulate fluid balance, nerve signaling, muscle contraction, cardiac conduction, and acid-base balance.
- This guide explains six commonly taught electrolytes: sodium, potassium, calcium, magnesium, phosphorus, and chloride.
- Electrolyte imbalances occur when levels are too low or too high and may cause symptoms such as weakness, cramps, confusion, irregular heartbeat, or neurologic changes.
- Lab results must be interpreted in context because normal ranges vary by laboratory and patient factors, medications, hydration status, kidney function, and symptoms all matter.
What Are Electrolytes and What Do They Do?
Electrolytes are minerals that carry an electrical charge when dissolved in body fluids. They are found in blood, urine, tissues, intracellular fluid, and extracellular fluid. Because they exist as charged ions, electrolytes help cells communicate, muscles contract, nerves fire, and fluid move between body compartments.
At a high level, electrolytes help regulate hydration and fluid balance, nerve signaling, muscle contraction, cardiac conduction, acid-base balance, and movement of nutrients and waste across cell membranes.
The important learning points for electrolytes include:
- Sodium, potassium, calcium, magnesium, phosphorus, and chloride
- The normal values clinicians commonly review for each electrolyte
- The major contributors to electrolyte imbalance
- Unique signs and symptoms of electrolyte imbalance
The key electrolyte components covered in this guide are sodium, potassium, calcium, magnesium, phosphorus, and chloride. These six values are commonly emphasized in nursing, ACLS, emergency care, and general clinical education. Other commonly measured electrolyte-related values also matter, including bicarbonate or carbon dioxide (CO2), especially when evaluating acid-base balance.
Key Terms to Know
- Electrolyte: a charged mineral that helps regulate body functions when dissolved in fluid.
- Ion: an atom or molecule with an electrical charge.
- Cation: a positively charged ion, such as sodium, potassium, calcium, or magnesium.
- Anion: a negatively charged ion, such as chloride, bicarbonate, or phosphate.
- Hyper-: a prefix meaning higher than normal.
- Hypo-: a prefix meaning lower than normal.
- pH: a measure of acidity or alkalinity; normal blood pH is commonly taught as about 7.35–7.45.

The basic metabolic panel is a blood test that measures electrolytes, glucose, and kidney function.
What is an Electrolyte Imbalance and How is it Tested?
An electrolyte imbalance occurs when an electrolyte level is too low or too high. Common contributors include vomiting, diarrhea, sweating, dehydration, overhydration, kidney dysfunction, heart disease, diabetes, malabsorption, and medications such as diuretics, antacids, steroids, antibiotics, chemotherapy medicines, or blood pressure medicines.
Symptoms vary by the electrolyte involved and by how quickly the imbalance develops. General symptoms may include weakness, fatigue, headache, nausea, vomiting, diarrhea, constipation, muscle cramps, spasms, numbness, tingling, confusion, irritability, or an irregular or fast heartbeat.
Red flags include seizures, severe confusion, fainting, severe weakness, chest pain, severe shortness of breath, new arrhythmia, inability to keep fluids down, severe dehydration, or symptoms in a patient with kidney disease, heart disease, diabetes, or medication changes.
How Electrolytes Are Tested
Electrolytes are usually checked with a blood test. A basic metabolic panel (BMP) commonly includes sodium, potassium, chloride, carbon dioxide or bicarbonate, calcium, glucose, BUN, and creatinine. A comprehensive metabolic panel (CMP) includes many of the same values and adds liver and protein-related tests. A standalone electrolyte panel may focus more directly on electrolytes such as sodium, potassium, chloride, bicarbonate, calcium, magnesium, and phosphate, depending on the laboratory and ordering system.
What Type of Results Will I Get?
Results are usually reported with a number, a unit, and a reference range. Common units include mEq/L, mmol/L, and mg/dL. Reference ranges vary by lab, patient population, test method, and specimen type, so clinicians should compare results with the range printed on the patient’s actual report.
Does a normal result mean everything is fine? Not always. A normal value can be reassuring, but it does not replace clinical judgment. Symptoms, medication history, kidney function, hydration status, acid-base status, ECG findings, repeat labs, and the direction of change over time may all affect interpretation.
6 Main Types of Electrolytes
This section explains six electrolytes commonly emphasized in clinical education: sodium, potassium, calcium, magnesium, phosphorus, and chloride. Each electrolyte has a typical reference range, key functions, and low or high imbalance patterns.
The ranges below are common teaching ranges, but actual reference intervals vary by laboratory and patient context.
| Electrolyte | Common teaching range | Low level | High level |
|---|---|---|---|
| Sodium | 135–145 mEq/L | Hyponatremia | Hypernatremia |
| Potassium | 3.5–5.0 mEq/L | Hypokalemia | Hyperkalemia |
| Calcium | 8.6–10.3 mg/dL | Hypocalcemia | Hypercalcemia |
| Magnesium | 1.7–2.2 mg/dL | Hypomagnesemia | Hypermagnesemia |
| Phosphorus | 2.5–4.5 mg/dL | Hypophosphatemia | Hyperphosphatemia |
| Chloride | 95–105 mmol/L | Hypochloremia | Hyperchloremia |
Sodium
Sodium is a major extracellular electrolyte involved in fluid balance, serum osmolality, nerve signaling, and muscle function. A standard sodium range is commonly taught as 135 to 145 mEq/L, though reference ranges vary between institutions.

Sodium is an essential electrolyte involved in nerve impulses, muscle function, and fluid balance.
Primary Functions
Sodium helps conduct nerve impulses and supports normal muscle function. It is also a major contributor to serum osmolality, which means the concentration of dissolved particles in the blood.
Sodium balance is tightly linked to water movement. When sodium concentration changes, water shifts between the vascular space and cells, which can affect thirst, blood volume, neurologic function, and overall hydration status.
Sodium balance is also influenced by the RAAS, which helps regulate fluid retention and vascular tone. Sodium, glucose, and other dissolved particles contribute to osmolality, so interpretation should consider the full clinical picture.
Hyponatremia
Hyponatremia is a sodium level below 135 mEq/L. One common pattern is dilutional hyponatremia, where excess water lowers the sodium concentration in the blood.
Congestive heart failure, kidney failure, and syndrome of inappropriate antidiuretic hormone (SIADH) may contribute to low sodium patterns. For a detailed comparison of fluid balance disorders, see diabetes insipidus vs SIADH.
Low sodium can affect the nervous system and may cause muscle cramps, weakness, confusion, headache, seizures, or worsening mental status. These neurologic symptoms are red flags within the broader electrolyte imbalance framework because rapid shifts in sodium and osmolality can be dangerous.
When serum sodium is low, serum osmolality may drop. Water can move from the vascular space into cells, which may contribute to cerebral swelling, cerebral edema, and seizures in severe or rapidly developing cases.
Hypernatremia
Hypernatremia is a sodium level over 145 mEq/L. It often reflects a water deficit relative to sodium, which can occur with dehydration, inadequate water intake, excessive water loss, osmotic diuresis, fever, or other clinical states.
Vomiting may contribute to dehydration and hemoconcentration in some patients, but it should not be presented as a direct or universal cause of hypernatremia. Clinicians should interpret hypernatremia with the patient’s volume status, urine output, medications, kidney function, glucose level, and overall clinical context.
Potassium
The normal potassium range is commonly taught as 3.5 to 5.0 mEq/L, though ranges vary across institutions. Most potassium is inside cells, while a smaller amount circulates in the blood, so even small serum changes can matter clinically.

The sodium-potassium pump helps move potassium into cells.
Primary Functions
Potassium is essential for:
- Cardiac function
- Nerve conduction
- Muscle contraction
Read: Electrocardiogram Interpretation in 10 Simple Steps
Hypokalemia
Hypokalemia is a low serum potassium level, commonly below 3.5 mEq/L. Contributing factors may include loop diuretics such as furosemide (Lasix®), gastrointestinal losses, poor intake, insulin therapy, beta-agonists such as albuterol, alkalosis, and intracellular potassium shifts.
Insulin stimulates potassium movement into cells. Inhaled albuterol can also shift potassium into cells, so patients receiving repeated breathing treatments may need potassium monitoring depending on the clinical context.
As a simplified teaching principle, hemodilution has a stronger direct effect on measured sodium concentration than on total-body potassium status. However, potassium interpretation still requires clinical context because serum potassium reflects a small extracellular fraction and can be influenced by shifts, kidney function, medications, acid-base status, and sampling factors.
Hyperkalemia
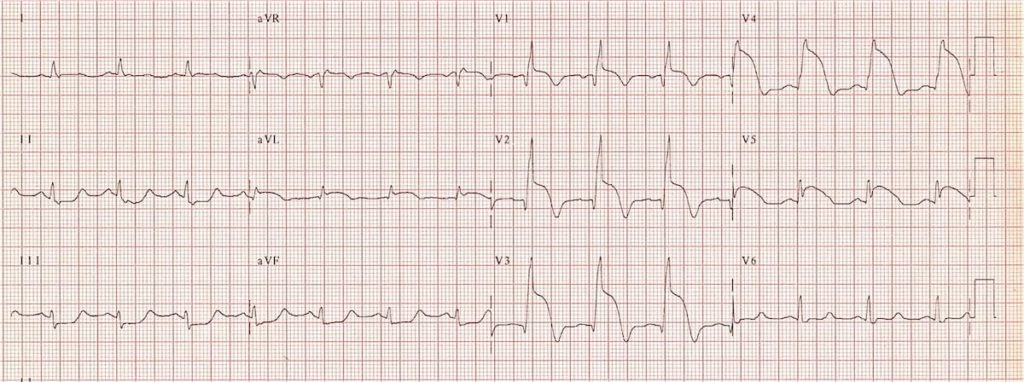
Hyperkalemia is a potassium level above the lab’s upper reference range. It may cause ECG changes, including peaked T waves, widening QRS, conduction delays, or dangerous arrhythmias depending on severity and rate of rise.
Major contributors include kidney dysfunction, ACE inhibitors, angiotensin II receptor blockers, potassium-sparing medications, rhabdomyolysis, hemolysis, metabolic acidosis, and tissue breakdown.
Lab context matters: potassium may be falsely elevated if the sample is hemolyzed or collected under difficult conditions. Clinicians should compare the lab result with symptoms, ECG findings, kidney function, medications, and whether the value needs repeat confirmation.
Hs and Ts – Hypo-Hyper Kalemia
This video reviews hypokalemia and hyperkalemia as reversible ACLS causes. Watch it after reading the potassium section if you want to connect potassium abnormalities with ECG changes and cardiac arrest management.
Calcium
The normal value for calcium is 8.6 to 10.3 mg/dL, however the range varies.
Lab context matters: many panels report total calcium, but ionized calcium is the biologically active “free” calcium. Albumin level, pH, kidney function, symptoms, and whether the lab reports total or ionized calcium can affect interpretation.
Primary Functions
Calcium has several important bodily functions:
- Bone metabolism: 99% of calcium is in bones and teeth.
- Blood coagulation: Calcium has a major role in the formation of prothrombin.
- Muscle contraction.
Hypocalcemia
Hypocalcemia is a low calcium level. A classic sign is tetany, meaning involuntary, repetitive muscle contractions or spasms caused by increased neuromuscular irritability. Other symptoms may include muscle cramps, weakness, tingling, seizures in severe cases, or hypotension depending on the clinical context.
Renal failure is the main contributor to hypocalcemia. The kidneys play a large role in vitamin D synthesis, and the body requires vitamin D to absorb calcium. If the kidneys are not properly synthesizing vitamin D, the body cannot absorb calcium and hypocalcemia presents.
Calcium levels also decrease in renal failure due to phosphorus build-up. Phosphorus levels increase as calcium levels decrease.
Hypercalcemia
Hypercalcemia is a high calcium level. The main signs are bone pain, kidney stones, abdominal pain, and confusion.
The main contributor to hypercalcemia is hyperparathyroidism. The parathyroid glands secrete parathyroid hormone (PTH), increasing calcium levels. If a patient has overactive parathyroid glands, calcium levels elevate.

The parathyroid glands secrete parathyroid hormone (PTH) to increase serum calcium levels.
Magnesium
The normal value for magnesium is 1.7 to 2.2 mg/dL, though it varies. Magnesium resides mostly in the bone and intracellular fluid and is primarily eliminated via the kidneys.
Primary Functions
Magnesium is important because it:
- Maintains cardiac rhythm
- Acts at neuromuscular junctions to facilitate nerve impulses
Magnesium plays a major role in cardiac rhythm. In dysrhythmia evaluation, potassium and magnesium are often reviewed together because both can affect myocardial excitability and conduction. If potassium is acceptable but rhythm concerns continue, magnesium is a common next electrolyte to assess.
Hypomagnesemia
Hypomagnesemia is a low magnesium level. Patients are often asymptomatic in mild cases. The main contributor to hypomagnesemia is alcoholism. Other causes are diarrhea and decreased absorption in the gastrointestinal tract.
Hypermagnesemia
Hypermagnesemia is a high magnesium level. The main symptoms are lethargy, weakness, and arrhythmias. The main contributor is renal failure. Since magnesium is primarily eliminated by the kidneys, patients with renal failure are not able to get rid of magnesium, so it builds up in the body.
Magnesium: ACLS Medications
This video explains magnesium’s ACLS medication role, including how it relates to rhythm management and selected dysrhythmia scenarios. It fits here because magnesium is clinically important when evaluating cardiac rhythm disturbances.
Phosphorus
The normal phosphorus range is 2.5 to 4.5 mg/dL. When phosphorus is a charged ion, it’s known as phosphate. The majority of phosphate is contained in the bones.
Primary Functions
The main functions of phosphorus are:
- Cellular metabolism: Phosphorus helps produce adenosine triphosphate (ATP).
- Formation of bone.
- Components of phospholipids and nucleic acids.

Phosphate is part of the adenosine triphosphate (ATP) molecule. The phosphate molecules are on the left side of the image.
Hypophosphatemia
Hypophosphatemia is a phosphorus level below 2.5 mg/dL. Patients are usually asymptomatic with mild to moderate hypophosphatemia. Patients with severe hypophosphatemia are weak due to ATP depletion.
The main contributors are malabsorption, diarrhea, and antacids. For example, a patient with malabsorption may have a partially removed intestine due to gastric bypass surgery. They can’t effectively absorb nutrients. For antacids, many aluminum and magnesium-based antacids bind to phosphate.
Clinical pearl: calcium and phosphorus often move in opposite directions, especially in kidney disease and parathyroid-related disorders. Interpret the relationship with kidney function, calcium level, vitamin D status, PTH, symptoms, and the patient’s overall lab pattern.
Hyperphosphatemia
Hyperphosphatemia is a high phosphorus level over 4.5 mg/dL. The main symptoms are calcium-phosphate precipitation in the joints, skin, heart, lungs. Some patients may develop hypocalcemia and subsequent tetany.
The main contributor is renal failure. The kidneys normally excrete phosphate. As kidney function worsens, so does its ability to excrete phosphate. Patients cannot properly filter out phosphorus.

As kidney function decreases, so does the ability to filter and eliminate various electrolytes in the body, especially phosphorus and calcium.
Chloride
Chloride is an often forgotten yet important electrolyte. A normal chloride level is between 95 to 105 mmol/L.
Primary Functions
Chloride’s main functions are:
- Acid-base balance: Chloride is part of hydrochloric acid, contributing to acidity in the body.
- Fluid balance.
Chloride and sodium have a complementary relationship. Sodium (Na+) has a positive charge, while chloride (Cl–) has a negative charge, so they are often discussed together in fluid and electrolyte balance.
Chloride also connects to acid-base balance because it interacts with bicarbonate and other buffers that help maintain pH. This is why chloride abnormalities are often interpreted alongside CO2/bicarbonate, sodium, anion gap, kidney function, and the patient’s clinical condition.
Hypochloremia
Hypochloremia is a low chloride level. Its main contributors are prolonged vomiting, diarrhea, and alkalosis.
Hyperchloremia
Hyperchloremia is a high chloride level. It may occur with dehydration or hemoconcentration, certain acid-base disorders, kidney dysfunction, large-volume chloride-rich IV fluids, medication effects, or other clinical conditions. Interpretation should be paired with sodium, bicarbonate or CO2, anion gap, kidney function, fluid status, and pH-related findings.
Summary
Electrolytes are charged minerals in body fluids that help regulate hydration, nerve signaling, muscle contraction, cardiac conduction, and acid-base balance. This guide focuses on six commonly taught electrolytes: sodium, potassium, calcium, magnesium, phosphorus, and chloride, while also noting that related values such as bicarbonate or CO2 may be measured on electrolyte panels, BMPs, or CMPs.
Low or high electrolyte levels can develop from fluid loss, overhydration, kidney dysfunction, medications, acid-base disorders, endocrine problems, or other illnesses. Symptoms can range from mild weakness or cramps to confusion, seizures, arrhythmias, or serious clinical deterioration.
The next step is to review the patient’s actual lab reference range, symptoms, medications, hydration status, kidney function, ECG findings when relevant, and trend over time. Seek urgent care for severe neurologic symptoms, fainting, chest pain, new arrhythmia, severe weakness, or inability to keep fluids down.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
Download the Acute Coronary Syndrome Managing STEMI PDF and view the videos to learn the treatment guidelines for managing STEMI.
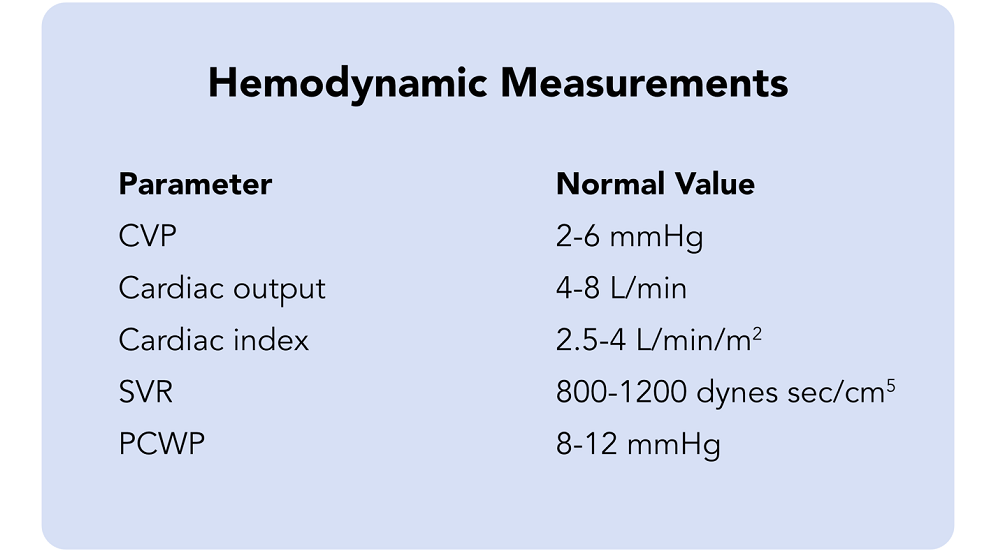
This article and video explore Hemodynamics. Learn the common hemodynamic measurements and the factors affecting...