Treating Reversible Causes of Pulseless Electrical Activity and Asystole
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- When a patient in asystole or pulseless electrical activity (PEA) does not improve after two minutes of high-quality CPR, it is essential to consider what may have caused the cardiac arrest.
- The Hs and Ts mnemonic assists providers in remembering the common and treatable causes of PEA and asystole.
- Should a patient achieve return of spontaneous circulation (ROSC), post-cardiac arrest care measures should be undertaken.
- Terminating resuscitative efforts may be considered when prolonged resuscitation does not lead to ROSC.

Adult Cardiac Arrest Algorithm
Read: Basic Life Support for Healthcare Providers
PEA is often caused by medical conditions that can be reversed.1 The provider must identify these conditions immediately, and interventions must occur as soon as possible. The provider should recall the Hs and Ts (refer to the Hs and Ts section of this course) when the patient’s condition does not improve after two minutes of CPR. The Hs and Ts mnemonic lists medical conditions that are likely to complicate cardiopulmonary resuscitation (CPR) efforts. For example, PEA is closely related to hypoxemia. An advanced airway, such as an endotracheal tube, must be inserted to improve oxygenation and ventilation. In this case, insertion of an endotracheal tube is the priority rather than defibrillation. An endotracheal tube may be inserted to improve oxygenation. PEA is also observed in other medical conditions leading to cardiac arrest, such as in severe hypovolemic shock and septic shock. In these conditions, intravenous or intraosseous fluid resuscitation therapy with a crystalloid solution is a priority, rather than defibrillation or securing an advanced airway. When pulmonary embolism or myocardial infarction is suspected to have caused the cardiac arrest, empirical fibrinolytic therapy might be considered the priority.2 Tension pneumothorax also causes PEA. In this case, needle thoracostomy to evacuate the trapped air within the thoracic cavity is a priority, followed by insertion of chest tubes for definitive management. Sometimes, echocardiography helps providers assess and guide the management of PEA. A cardiac ultrasound can detect cardiac tamponade, intravascular volume status, mass lesions, blood clots, left ventricular contractility, regional wall motion abnormalities, and ventricular volume. Asystole, on the other hand, is an end-stage rhythm secondary to prolonged ventricular fibrillation (VF) and PEA. The prognosis for asystole is very poor.Hs and Ts

Once the patient has achieved ROSC, post-cardiac arrest care is initiated (see the article on post-cardiac arrest care). Post-cardiac arrest care concentrates on treating hypoxemia, maintaining blood pressure, and continuing interventions for the underlying cause of the cardiac arrest. If a patient is comatose after ROSC, providers should apply targeted temperature management (TTM). Increased survival rates to hospital discharge with good neurological outcomes have been observed when TTM is provided.ROSC After PEA and Asystole
Related Video – Understanding the Post Cardiac Arrest Algorithm
It is justifiable to withdraw resuscitative efforts when multiple variables prognosticate a poor outcome during cardiac arrest. If a patient is intubated, not achieving an end-tidal CO2 greater than 10 mm Hg via waveform capnography after 20 minutes of CPR is one such variable for withdrawing resuscitative efforts.3 However, this parameter must not be used alone. There are very few studies and criteria that accurately predict the outcome of continued resuscitation when the situation might be considered futile. Therefore, all cardiac arrest patients must undergo CPR unless an advanced directive or a Do Not Resuscitate (DNR) order is in place or in the presence of irreversible death (such as a patient who has been decapitated or exhibits dependent lividity).Terminating Resuscitative Efforts
When a patient in asystole or PEA does not improve after two minutes of high-quality CPR, it is important to evaluate the cause of the cardiac arrest. The Hs and Ts mnemonic can help identify potentially reversible causes of cardiac arrest, but there are also times when the provider will need to terminate resuscitative efforts.Summary
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
1. Sandy N Shah, DO, MBA, FACC, FACP, FACOI; Chief Editor: Jose M Dizon, MD. Pulseless Electrical Activity. MedScape. 2018.
2. Eric J. Lavonas, Chair; Ian R. Drennan; Andrea Gabrielli; Alan C. Heffner; Christopher O. Hoyte; Aaron M. Orkin; Kelly N. Sawyer; Michael W. Donnino. Special Circumstances of Resuscitation. American Heart Association. 2015.
3. American Heart Association. Adult Advanced Cardiovascular Life Support. 2015.
More to Learn
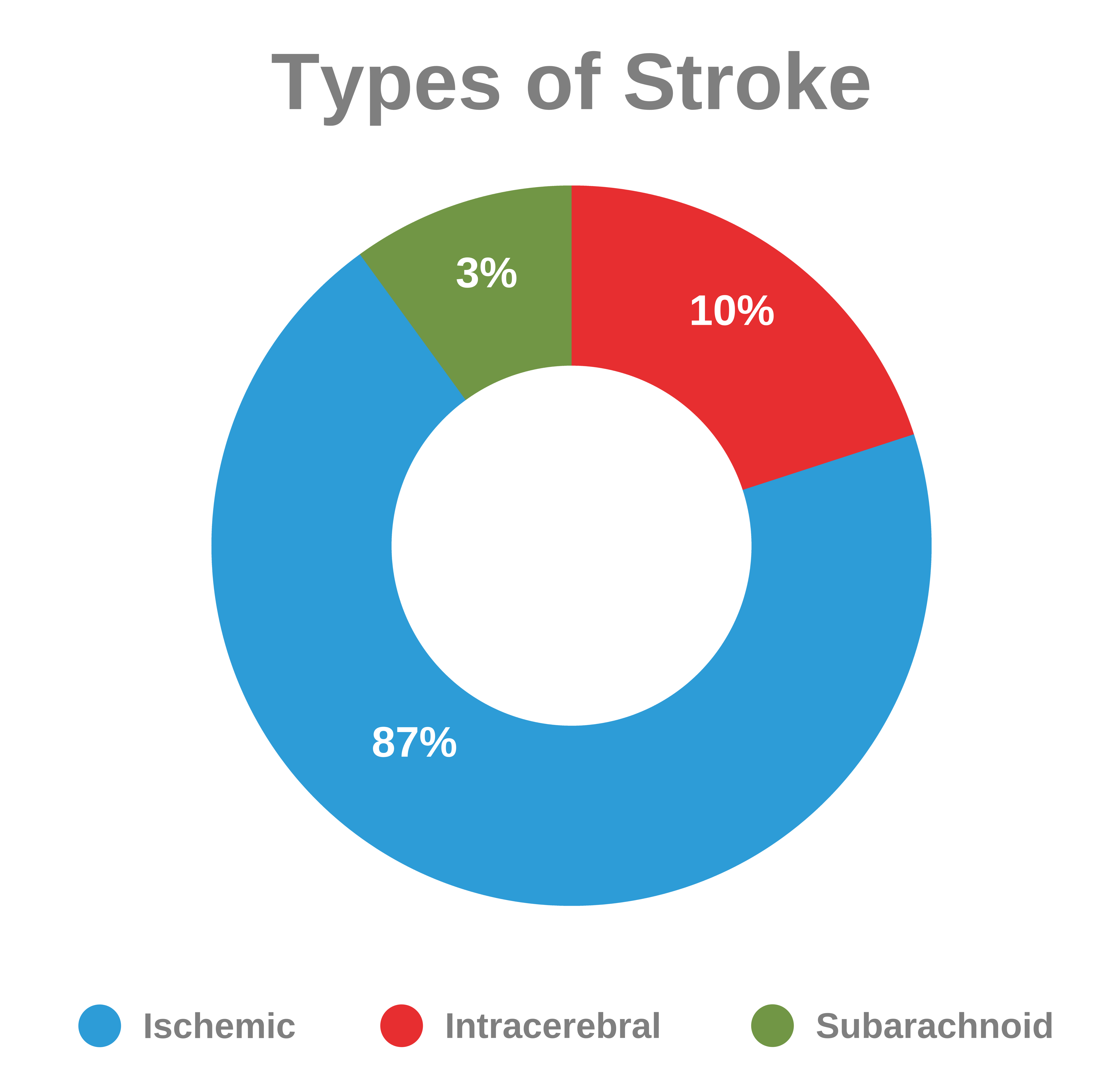
Learn to simplify the Assessment, Important Time-Frames and Clinical Diagnosis of acute stroke patients for ACLS providers, which is especially useful in the out-of-hospital situation.
Gain insights into effective ACLS treatments for tension pneumothorax, a critical condition, by reading our article. Learn about life-saving interventions for this lung-related emergency.