Immediate Post-Cardiac Arrest Care
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Table of Contents
- Immediate Post-Cardiac Arrest Care Algorithm
- Initial Stabilization Post-Cardiac Arrest
- Ongoing Assessment and Management Post-Cardiac Arrest
- Coronary Angiography
- Does the Patient Follow Commands?
- Targeted Temperature Management
- Continuing Temperature Management Beyond 24 Hours
- Out-of-Hospital Cooling
- Hemodynamic Goals after Resuscitation
- Prognostication after Cardiac Arrest
- Organ Donation
- American Health Association Immediate Post-Cardiac Arrest Algorithm
- Optimizing Ventilation and Oxygenation
- Cardiovascular Care
- Targeted Temperature Management
Article at a Glance
- Post-cardiac arrest care begins as soon as the patient achieves return of spontaneous circulation (ROSC).
- Care must be taken to avoid hyperoxygenation and hyperventilation in the intubated patient on mechanical ventilation.
- Patients with ST elevation myocardial infarction (STEMI) should undergo revascularization procedures, including those who are comatose.
- Hypotension must be addressed immediately in the post-cardiac arrest period. Hypertension is treated with vasopressors.
- Targeted temperature management (TTM) can prevent further neurological damage after cardiac arrest.
Immediate Post-Cardiac Arrest Care Algorithm

Immediate Post-Cardiac Arrest Care Algorithm
Post-cardiac arrest care begins immediately after the patient experiencing cardiac arrest achieves return of spontaneous circulation (ROSC).1 It involves two phases: 1) initial assessment and management, and 2) ongoing assessment and management.
In the initial stabilization phase, the emphasis is on optimizing ventilation and oxygenation and the treatment of hypotension. During this phase, the team must manage the airway, obtain an electrocardiogram (ECG), initiate waveform capnography, and titrate oxygen to achieve an oxygen saturation from 92% to 98% and a partial pressure of carbon dioxide of 35–45 mm Hg. The respiratory rate can be started at 10 breaths per minute but should be increased or decreased based on the patient’s response. The patient’s blood pressure (BP) should be maintained with a systolic BP > 90 mm Hg or a mean arterial pressure (MAP) > 65 mm Hg. The team can administer crystalloid fluids or vasopressors or inotropes to increase the BP, often targeting the RAAS pathway that regulates vascular tone and fluid balance.Initial Stabilization Post-Cardiac Arrest
Once the patient is stabilized, the team must continue to provide ongoing assessment and manage the patient’s care. The elements of this phase are detailed below.Ongoing Assessment and Management Post-Cardiac Arrest
If a patient is suspected of having ST elevation myocardial infarction (STEMI), unstable cardiogenic shock, or if mechanical support is required in the prehospital setting, then emergency coronary angiography should be considered. It can be performed even if the patient is comatose. Studies show that increased rates of survival are achieved in patients who undergo emergency coronary revascularization procedures. Coronary Angiography
If the patient is awake, the team should provide other critical care management. If the patient is comatose, the team should implement targeted temperature management (TTM), obtain a computed tomography (CT) of the brain, provide ongoing electroencephalogram (EEG) monitoring, along with providing other critical care management.Does the Patient Follow Commands?
Post-cardiac arrest patients who are comatose must undergo TTM. That involves using various measures, such as a cooling blanket, to maintain a core temperature of 32–36°C for 24 hours.2Targeted Temperature Management
Fever must be prevented or controlled in post-cardiac arrest patients because a high core temperature is closely related to neurologic injury in patients who are comatose. Providing antipyretics will not hinder any treatments provided to patients receiving advanced critical care.Continuing Temperature Management Beyond 24 Hours
Emergency services must refrain from providing rapid infusion therapy with cold intravenous fluids if the patient has achieved ROSC in the field. There are possible complications that can develop from doing so, and these complications are better addressed in a critical care setting.Out-of-Hospital Cooling
Corrective treatment of hypotension is indicated in post-cardiac arrest patients with a systolic blood pressure of less than 90 mm Hg and a diastolic blood pressure of less than 65 mm Hg. Hypotension is linked to higher mortality rates and diminished functional recovery.Hemodynamic Goals after Resuscitation
Read: Interpreting an ECG Strip
Prognostication and assessing the neurologic outcome for the comatose patient is best performed 72 hours after cardiac arrest. When a patient has undergone TTM or has been sedated, prognostication can start 72 hours after the patient has returned to normal body temperature or after the effects of sedation have waned.Prognostication after Cardiac Arrest

Postcardiac Arrest Standards of Care
It is recommended that all patients who have been diagnosed with brain death undergo evaluation for possible organ donation. There is no documented difference in outcomes if an organ transplanted to a patient came from a post-cardiac arrest patient or a healthy patient.Organ Donation
Immediate Post-Cardiac Arrest Algorithm
Immediate Post-Cardiac Arrest Care Algorithm
The goal of post-cardiac arrest care is to improve the outcomes of patients achieving ROSC.3 The algorithm guides the clinician in performing post-cardiac arrest care. Pediatric patients require age-specific resuscitation strategies, which are outlined in the PALS Post-Cardiac Arrest Algorithm used for ongoing stabilization and neurologic management after ROSC. It involves a multidisciplinary approach and requires several specialists to work together for the survival of the patient with an optimal neurologic outcome.
If there is cardiovascular dysfunction from an acute cardiac etiology, for example, then these patients must have ventilatory support and close monitoring of circulation using vasopressors and other interventions to address cardiac dysfunction. If there is severe neurological dysfunction (such as coma), the patient must undergo TTM.
Related Video – Understanding the Adult Immediate Post-Cardiac Arrest Care Algorithm
Excessive ventilation and hyperoxygenation should be avoided in the post-cardiac arrest patient on a mechanical ventilator. Hyperventilation and excessive oxygenation are associated with increased morbidities and mortality. Hyperventilation constricts cerebral blood vessels as a compensatory mechanism from a decrease in arterial carbon dioxide concentration. It can also increase intrathoracic pressure that may inhibit the circulation in the mediastinum. It can also cause volutrauma or tension pneumothorax. The rate of ventilation can be titrated to achieve end-tidal carbon dioxide pressures between 35 mm Hg and 45 mm Hg. Hyperoxygenation can cause oxygen toxicity-induced reperfusion injuries in the post-cardiac arrest period, as too much oxygen precipitates free radicals that can potentially harm cells. Oxygen supplementation must be titrated to achieve an oxygen saturation between 92% and 98%. Post-cardiac arrest care includes optimizing ventilation and oxygenation for patients on a mechanical ventilator.Optimizing Ventilation and Oxygenation

If a patient is suspected of having acute coronary syndrome, then it is necessary to perform ancillary testing to make the diagnosis and perform prompt interventions. A 12-lead electrocardiogram (ECG) must be obtained to determine if the patient has experienced STEMI.4 If the patient has experienced STEMI, they immediately undergo angiography with possible recanalization therapy of the diseased coronary artery. Acute coronary syndromes are common in the prehospital setting. Studies have shown that 96% of patients with STEMI will have a coronary artery lesion, while only 58% of patients without STEMI will have a coronary artery lesion.5 Selected patients with non-ST segment elevation myocardial infarction (NSTEMI) should also undergo invasive treatments. These interventions can be performed in patients who are comatose after ROSC. There are no blood pressure goals in these patients, except for immediate treatment of hypotension (systolic blood pressure < 90 mm Hg or diastolic blood pressure < 65 mm Hg). Vasopressors are used to improve cardiac output and, subsequently, perfusion to the heart and brain. Vasopressors have positive chronotropic effects to improve heart rate, inotropic effects to improve myocardial contractility, and vasoconstrictive and vasodilatory effects to improve arterial pressure or reduce afterload, respectively. Clinicians must carefully balance these medications. Therefore, close monitoring of the patient’s hemodynamic status is necessary. These drugs are titrated to achieve the desired effect. The following medications are the common vasoactive drugs used to treat patients post-cardiac arrest:Cardiovascular Care
Common Vasoactive Drugs

Vasopressors, such as epinephrine and dopamine, are given intravenously.
Related Video – Epinephrine – ACLS Drugs
The goals of targeted temperature management (TTM) are to induce hypothermia between 32°C and 36°C for at least 24 hours to improve the neurologic function of the patient who is comatose. TTM can be deferred in certain situations, such as acute bleeding.6 However, it is a priority if a post-cardiac arrest patient is prone to seizures or has cerebral edema. After completing TTM, fever must be strictly controlled. Fever is associated with worsening of neurologic dysfunction and patient outcome. Post-cardiac arrest care begins as soon as the patient achieves ROSC and includes initial assessment and management and ongoing assessment and management.Targeted Temperature Management
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
1. Mary Ann Peberdy, Clifton W. Callaway, Robert W. Neumar, Romergryko G. Geocadin, Janice L. Zimmerman, Michael Donnino, Andrea Gabrielli, Scott M. Silvers, Arno L. Zaritsky. Post-Cardiac Care. American Heart Association. 2010.
2. Ahmad M. Omairi; Shivlal Pandey. Targeted Hypothermia Temperature Management. National Library of Medicine. 2021.
3. Stephen Pfeiffer, MD, Matthew Zackoff, MD, MEd, Katelyn Bramble, RN, Lindsey Jacobs, RN. Care Does Not Stop Following ROSC: A Quality Improvement Approach to Postcardiac Arrest Care. Pediatric Quality & Safety. 2021.
4. Oren J. Mechanic; Michael Gavin; Shamai A. Grossman. Acute Myocardial Infarction. National Library of Medicine. 2022.
5. Liza Chacko, James P. Howard, Christopher Rajkumar, Alexandra N. Nowbar, Christopher Kane, Dina Mahdi, Michael Foley, Matthew Shun-Shin, Graham Cole. Effects of Percutaneous Coronary Intervention on Death and Myocardial Infarction Stratified by Stable and Unstable Coronary Artery Disease. American Heart Association. 2020.
6. Peggy L. Nguyen, Laith Alreshaid, Roy A. Poblete, Geoffrey Konye, Jonathan Marehbian, and Gene Sung. Targeted Temperature Management and Multimodality Monitoring of Comatose Patients After Cardiac Arrest. Frontiers in Neurology. 2018.
More to Learn
Master injectables calculations with our comprehensive guide. Learn the formula for accurate drug calculations to ensure precise medication administration.
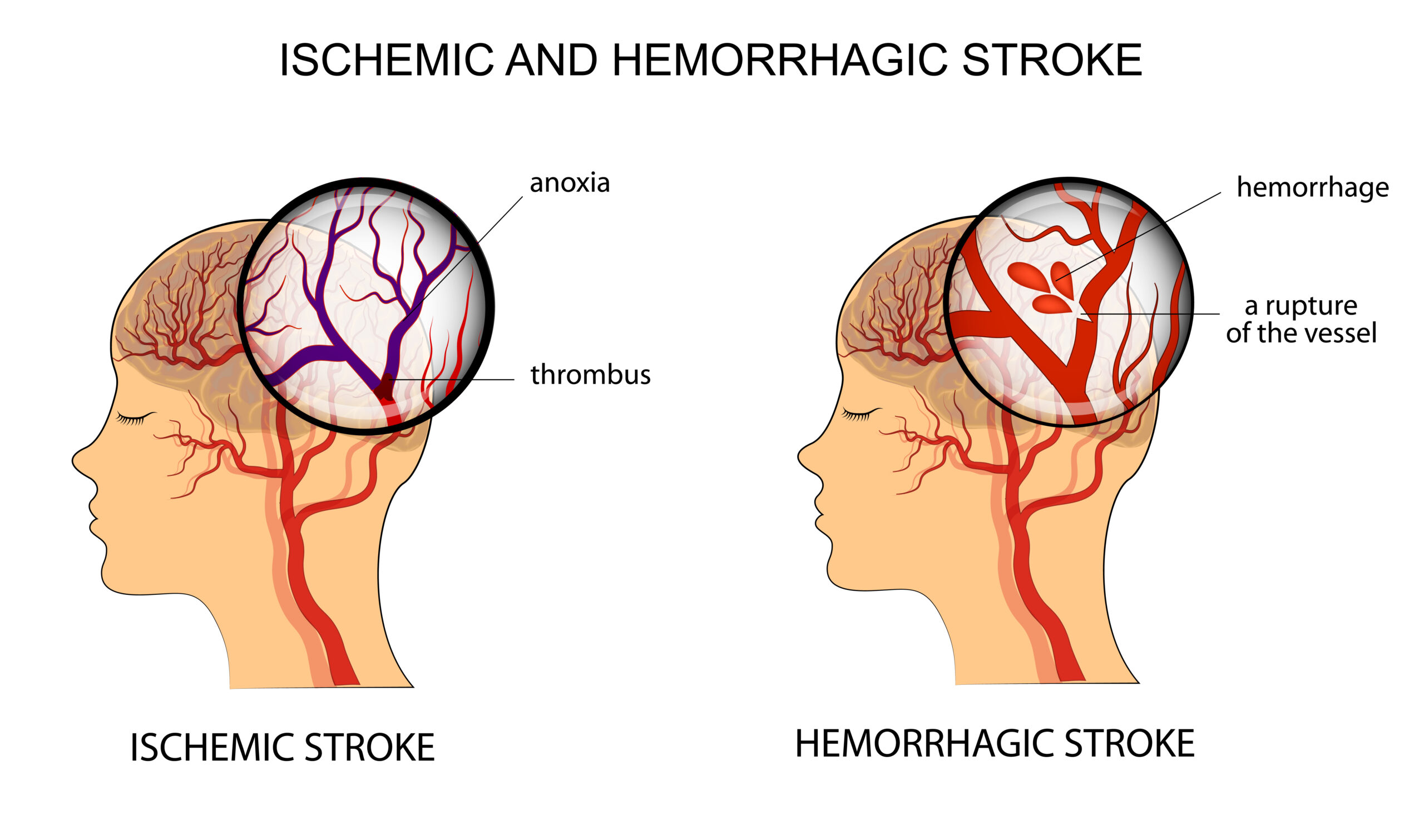
Learn the process of Acute Stroke Assessment in the Emergency Department. The general assessment is followed by Neurological assessment and determining ischemic or hemorrhagic stroke.