HHS vs. DKA: Understanding the Differences
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Hyperosmolar hyperglycemic syndrome is a complication of type 2 diabetes.
- The blood glucose for hyperosmolar hyperglycemic syndrome is typically much higher than diabetic ketoacidosis.
- Clinicians will learn how hyperosmolar hyperglycemic syndrome differs from diabetic ketoacidosis.
Hyperosmolar hyperglycemic syndrome (HHS) is similar to diabetic ketoacidosis (DKA), but there are several differences we will review in this article. How common is HHS? HHS is less common than DKA and is estimated to account for less than 1% of hospital admissions in patients with diabetes. Patients with type 2 diabetes are at risk of HHS. Physicians must remember: HHS most often occurs in people with type 2 diabetes (including undiagnosed diabetes), especially when an illness or stressor causes severe dehydration and sustained hyperglycemia. Quick clinical reminder: HHS is classically linked to type 2 diabetes, while DKA is classically linked to type 1 diabetes—however, either condition can occur outside these “classic” patterns depending on the trigger and insulin availability. There are little to no ketone bodies in the blood in HHS since patients with type 2 diabetes have insulin in their bodies to protect against lipolysis. Lipolysis, or the breakdown of fat, leads to the build-up of ketone bodies present in DKA. A hallmark DKA symptom is the presence of ketone bodies. A type 1 diabetic does not produce insulin to bring glucose into the cells. Therefore, the cells do not have glucose available as an energy source, so the body breaks down fats instead via lipolysis. The extracellular fluid (ECF) of the vascular space with an HHS patient is extremely hyperosmolar due to elevated blood glucose. Osmolality (or colloid osmotic pressure) is created by albumin, glucose, sodium, and other components in the vascular space. Due to the hyperosmolar ECF, the body tries to dilute the blood to rid itself of the extra glucose. When glucose is removed through the urine, water follows. Therefore, patients with HHS are at risk of extreme dehydration due to water loss. Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic syndrome (HHS) both result from insulin deficiency, but the degree and metabolic consequences differ significantly. In DKA, an absolute or near-absolute lack of insulin leads to unchecked lipolysis. Fat breakdown produces ketone bodies, resulting in metabolic acidosis. This process occurs rapidly and is most common in patients with type 1 diabetes. In contrast, HHS occurs in the presence of relative insulin deficiency. There is enough insulin to suppress ketone formation but not enough to prevent severe hyperglycemia. Profound hyperosmolarity develops, causing osmotic diuresis, extreme dehydration, and altered mental status. Although both conditions are medical emergencies, treatment priorities differ slightly between DKA and HHS. DKA is characterized by hyperglycemia, metabolic acidosis, and ketonemia, whereas HHS is defined by extreme hyperglycemia, high serum osmolality, and minimal or absent ketosis. While laboratory thresholds differ, clinical context and overall presentation guide diagnosis and management decisions. Blood contains components such as albumin (protein), glucose, and sodium that contribute to the osmotic pressure of the blood. Read: Coronary Artery Disease vs. Peripheral Artery Disease The main concern with HHS is hypovolemia. Fluid replacement is crucial because osmotic diuresis is very severe in these patients. The polyuria from hyperglycemia causes osmotic diuresis. To compare HHS and DKA: Both diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic syndrome (HHS) are associated with serious complications if not treated promptly. While mortality is higher in HHS, both conditions can result in life-threatening outcomes. Early recognition and aggressive management significantly reduce the risk of these complications. Patients with HHS are constantly urinating and thirsty. They may become dehydrated. An HHS diagnosis indicates a blood glucose of over 600 mg/dL, whereas the diagnosis of DKA is a blood glucose of over 250 mg/dL. Patients with type 2 diabetes often get HHS. It frequently goes undiagnosed for years until the one day they wake up lethargic and dehydrated, indicating undiagnosed HHS and diabetes. Laboratory evaluation plays a central role in differentiating HHS from DKA and guiding treatment decisions. Additional laboratory testing may include serum creatinine, blood urea nitrogen (BUN), lactate, and infectious workup to identify precipitating factors. Sometimes people who present with HHS actually have undiagnosed type 2 diabetes. Type 1 diabetics are typically diagnosed at a very early age. They know how to monitor their sugar levels and when to seek treatment. But, if the patient is unaware of their diabetes, they may put off seeking treatment. Additionally, the appearance of the “3 Ps” which go with hyperglycemia are much more subtle with HHS patients than those with DKA. Sometimes, these patients may have a blood glucose 1200 mg/dL or higher. HHS is a complication of type 2 diabetes, while DKA is a complication of type 1 diabetes. Blood glucose levels in HHS patients will be very elevated compared to the levels of DKA patients. Hypovolemia is the main concern with HHS, while hypokalemia is the main concern with DKA. Hyperosmolar Hyperglycemic Syndrome
What Are the Risk Factors for Hyperosmolar Hyperglycemic State (HHS)?
DKA vs. HHS: A Detailed Comparison
Pathophysiology
Treatment Protocols
Diagnostic Criteria Overview

Fatal Complications of HHS

Related Video – What is Hyperosmolar Hyperglycemic Syndrome (HHS)?
Diagnostic Criteria and Lab Findings for HHS and DKA

Summary
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
Uncover the potential of Adenosine Injection in ACLS drug therapy for SVT. Our article details proper dosing and administration for effective life-saving interventions.
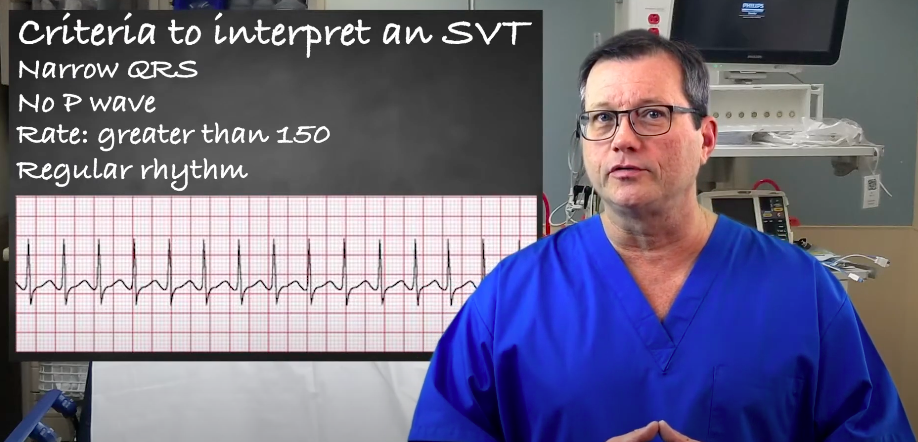
Understand the criteria and interpretation of supraventricular tachycardia (SVT) by reading our article. Learn to accurately identify and evaluate SVT.