Coronary Artery Disease vs. Peripheral Artery Disease
This article reviews the core concepts of coronary artery disease (CAD) and peripheral artery disease (PAD). Designed for nursing professionals and students, this guide covers the underlying pathophysiology, unique signs and symptoms, and crucial nursing interventions for both conditions. By the end of this article, you will understand how to distinguish these location-specific arterial diseases and evaluate their respective treatment options.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Table of Contents
- What’s the Difference?
- What is Coronary Artery Disease?
- Pathophysiology of CAD
- Symptoms of CAD
- Diagnosing CAD
- Nursing Care for CAD
- Treatments for CAD
- What is Peripheral Arterial Disease?
- Pathophysiology of PAD
- Clarifying the Difference between PAD and Peripheral Venous Insufficiency
- Symptoms of PAD
- Diagnosing PAD
- Nursing Care for PAD
- Treatments for PAD
- Can a Patient Have PAD and CAD?
- Summary
Article at a Glance
Here is a quick side-by-side comparison of these two distinct but related conditions:
- Location: CAD narrows the coronary arteries of the heart; PAD narrows the arteries in the peripheral extremities, particularly the legs.
- Hallmark Symptoms: CAD often presents as chest pain (angina); the classic sign of PAD is intermittent claudication (leg pain during exercise).
- Typical Tests: CAD relies on ECGs, stress tests, and coronary angiography; PAD relies on the Ankle-Brachial Index (ABI) and Doppler ultrasound.
- Typical Treatments: Both rely heavily on lifestyle changes and atherosclerosis management, though procedural interventions target the specific occluded vascular beds.
What’s the Difference?
While CAD and PAD are driven by the exact same underlying biological process, they are classified differently based on where the disease occurs in the body.
| Disease | Vascular Focus | Primary Danger |
| CAD | Coronary Arteries (Heart) | Acute Myocardial Infarction |
| PAD | Peripheral Arteries (Legs/Feet) | Critical Ischemia and Tissue Loss |
What is Coronary Artery Disease?
CAD is a progressive narrowing of the coronary arteries caused by atherosclerosis. Atherosclerosis is the pathological process where sticky fatty plaques build up within the inner lining of the arteries over time. While severe clinical symptoms (like angina) are often most noticeable when coronary arteries become significantly occluded, historically noted around 70% or higher, CAD is a progressive disease that begins long before flow-limiting blockages appear.

Coronary artery disease is the build-up of plaque in the coronary arteries.
Pathophysiology of CAD
To understand CAD, it is important to examine both the risk factors and the specific biological etiologies.
1. Risk Factors
- Smoking: Causes repeated inflammation that damages the lining of vessels.
- Hypertension: High blood pressure shears and damages the vessels over time.
- Diabetes: High blood glucose damages the vascular endothelium over time.
- Age: The risk increases with age (men over 45 and women over 55 are at higher risk).
- High Cholesterol: Also known as hyperlipidemia or dyslipidemia. High levels of low-density lipoprotein (LDL) heavily contribute to plaque formation.
- Family History: A genetic history of heart disease is a major risk factor.
2. The Inflammatory Cascade and Plaque Formation
Inflammation is biologically intended to heal and repair the body, but when triggered abnormally, it becomes harmful to the arteries. The risk factors listed above set off this inflammatory response in the lining of the coronary arteries.
When the inflammatory cascade is triggered, cytokines (signaling proteins) are released. These cytokines attract macrophages (specialized white blood cells), which stick to the damaged vessel site and ingest LDL cholesterol. This LDL cholesterol is sticky and harmful to the blood vessels, eventually leading to the formation of fatty streaks. Over time, these fatty streaks harden into fibrotic plaques, the hallmark of atherosclerosis.
(For further reading on arterial inflammation, consult the American Heart Association guidelines).
3. Plaque Rupture and Clot Formation
The ultimate concern in CAD is plaque rupture. If the fibrotic plaque breaks open, it triggers the body’s coagulation cascade:
- Thrombin (a clotting enzyme) is produced.
- Thrombin converts fibrinogen (a soluble protein in blood) into fibrin (an insoluble protein mesh).
- Platelets are attracted to this fibrin mesh, forming a thrombus (blood clot) inside the coronary artery.
This thrombus can cause partial or complete occlusion of the artery, leading to a heart attack (myocardial infarction or acute coronary syndrome).

Over time, injury to the arteries can lead to the development of plaques, or atherosclerosis.
The concern in CAD is if the fibrotic plaque ruptures and triggers the coagulation cascade. This causes a thrombus in the coronary arteries. The thrombus can potentially lead to partial or complete occlusion of the coronary artery, causing infarction, which is known as acute coronary syndrome or myocardial infarction. Management of this condition follows the acute coronary syndrome algorithm.
Symptoms of CAD
While CAD can be asymptomatic in its early stages, progressive occlusion eventually causes myocardial oxygen demand to exceed supply. The most common symptoms include chest pain (angina) or pressure, shortness of breath, unusual fatigue, and diaphoresis (sweating). Symptoms often worsen with physical exertion.
Diagnosing CAD
Diagnosing CAD requires a combination of clinical assessment and specific cardiac testing. Common diagnostic tools include 12-lead electrocardiograms (ECGs) to look for ischemic changes, stress tests (exercise or pharmacological), echocardiograms, and the gold standard: coronary angiography, which visually maps arterial blockages.
Nursing Care for CAD
Nursing management for CAD focuses on optimizing perfusion and minimizing cardiac workload. Key interventions include continuously monitoring vital signs and ECG rhythms, safely administering ordered cardiac medications (like beta-blockers and antiplatelets), and providing robust patient education on symptom recognition and crucial lifestyle modifications.
Treatments for CAD
The keystone of treatment for CAD is lifestyle changes, especially if it has not yet developed into a myocardial infarction. Some of the recommended lifestyle interventions include:
- Eating a heart-healthy diet that is low in cholesterol, sodium, and fat.
- Exercising for at least 30 minutes three times per week.
- Losing weight, if the patient is obese.
- Quitting smoking.
- Managing chronic conditions, such as hypertension and diabetes.
Medications used in the treatment of CAD include lipid-lowering agents and other cardiac drugs:
- Statins: The most widely used first-line class of cholesterol-lowering medications. While statins work exceptionally well to lower cholesterol, liver enzymes must be monitored routinely as they can affect hepatic function.
- Aspirin: Works as an antiplatelet to prevent clots and subsequent myocardial infarction.
- Other Antiplatelets: Clopidogrel (Plavix®) and ticagrelor (Brilinta®) work differently than aspirin. While traditionally patients are prescribed either aspirin or an antiplatelet (if they cannot tolerate aspirin), patients with a recent MI or coronary stent may be placed on Dual Antiplatelet Therapy (DAPT) combining both, per ACC/AHA guidelines.
- Nitrates: Nitroglycerin is commonly prescribed to cause rapid vasodilation, relieving angina by increasing blood flow and reducing myocardial oxygen demand.
- Beta-blockers: First-line antihypertensive agents in CAD that have been shown to decrease mortality. They help the heart fill during diastole, which decreases cardiac contractility and myocardial demand. For a deeper understanding of how these drugs compare, see beta agonists vs beta blockers.
- Bile acid resins: (e.g., Cholestyramine) Lower cholesterol by attaching to bile in the intestines, preventing fat absorption and passing it through stool. They must be taken with food and can interfere with the absorption of other drugs (take one hour before or four hours after other medications).
- Ezetimibe (Zetia®): Used alone or in addition to statins to help lower cholesterol.
- Niacin: A B-vitamin that lowers cholesterol but can cause facial flushing and warmth due to vasodilation.
Surgical Interventions: When lifestyle and medical management are insufficient, procedures such as Percutaneous Coronary Intervention (PCI/stenting) or Coronary Artery Bypass Grafting (CABG) are utilized to mechanically restore blood flow to the heart muscle.
Read: Hyperosmolar Hyperglycemic Syndrome: How Is It Different From DKA
What is Peripheral Arterial Disease?
Note: The terms “Peripheral Arterial Disease” and “Peripheral Artery Disease” are used interchangeably in clinical practice.
Peripheral arterial disease (PAD) is a circulatory problem caused by narrowed arteries. Unlike CAD, which attacks the heart, PAD specifically impacts the arteries in the peripheral extremities, particularly the legs, preventing them from receiving enough blood flow to meet metabolic demands.
Pathophysiology of PAD
The pathophysiology of PAD is fundamentally the same process as CAD. Because atherosclerosis is a systemic disease, the inflammatory plaque buildup that threatens the heart can also occur simultaneously in other vascular beds. The primary difference is simply which blood vessels are affected.
There are two classifications of PAD:
- Functional PAD. Functional PAD is characterized by intermittent claudication, the classic sign of PAD. The blood flow is good at rest, but ischemia occurs with exercise. Functional PAD is otherwise known as Stage II disease.
- Critical PAD. Critical PAD is characterized by pain at rest (Stage III disease). The final stage of PAD (Stage IV disease) is characterized by trophic skin changes, such as dryness, scaling, and lack of hair growth.
When a patient’s foot does not have adequate blood flow for a long period, the foot will not be healthy. It will lack hair, the skin will look flaky, and the toenails will dry and scale off.

Peripheral arterial disease is caused by atherosclerosis in the peripheral arteries.
Clarifying the Difference between PAD and Peripheral Venous Insufficiency
Because both conditions cause severe leg symptoms, they are commonly confused when evaluating a patient; therefore, it is vital to contrast them. PAD is a blood flow (arterial delivery) issue, while peripheral venous insufficiency is a blood return (venous drainage) issue.
In PAD, the body does not have adequate blood flow to the extremities. The classic hallmark symptom is intermittent claudication, though as the ischemia progresses, patients will experience paresthesia, neuropathic pain, and tingling. The skin is often pallor and cool to the touch, with low hair growth.
Another sign is pulselessness. It is usually difficult to find the pedal pulse and may require the use of a Doppler ultrasound. In a clinical setting, an Ankle-Brachial Index (ABI) test is heavily utilized to compare blood pressure in the ankle to the arm to confirm PAD.

Ulcers are common on the outside of the foot in peripheral arterial disease.
With peripheral venous insufficiency, blood is getting to the lower limb but not returning properly. The most common cause of venous insufficiency is varicose veins. Another cause is incompetent valves.
Signs and symptoms of peripheral venous insufficiency include edema, pain that improves when the legs are raised, a “messy” ulcer, and swelling. The ulcer may be brown in color with drainage. The ulcer will typically be located at the medial malleolus or the inside of the ankle.

Varicose veins are the most common cause of peripheral venous insufficiency.
Symptoms of PAD
Symptoms of PAD escalate in stages. Patients generally start with intermittent claudication (leg pain/cramping with exercise that stops with rest). As it progresses to Critical PAD, patients suffer pain at rest, followed by trophic skin changes (dry, scaling skin, loss of leg hair), and the development of non-healing, “punched out” arterial ulcers on the feet.
Diagnosing PAD
Providers diagnose PAD by assessing pedal pulses (often requiring a Doppler) and performing an Ankle-Brachial Index (ABI) test. Angiography or vascular ultrasounds may also be used to visualize the exact location and severity of the peripheral blockages.
Nursing Care for PAD
Since PAD is a blood flow issue, nursing care directly addresses perfusion:
- Keeping the legs below the level of the heart (dependent position) to make sure they are perfused with gravity’s assistance. Raising the legs might reduce the blood flow even more.
- Keeping the extremities warm with socks or gloves. A heating pad should not be used because patients, especially those with advanced peripheral neuropathy, may not be able to feel the heat to indicate if it is burning them.
Related Resource: Because PAD nursing care relies heavily on monitoring systemic perfusion, understanding Mean Arterial Pressure (MAP) is highly relevant. This video explains how to quickly calculate MAP to ensure your patient’s organs and extremities are receiving adequate blood flow.
Treatments for PAD
Effective PAD treatment consists of lifestyle interventions, medications, and potentially surgery. Lifestyle interventions for PAD are similar to those for CAD.
Lifestyle interventions that help manage and reduce the progression of PAD are:
- Quitting smoking
- Exercising
- Eating a healthy diet
Some medications used in the treatment of PAD include:
- Pentoxifylline (Trental®). Pentoxifylline helps to reduce blood viscosity. It helps the blood flow more easily through narrowed arteries.
- Cilostazol (Pletal®). Cilostazol is an antiplatelet drug and a vasodilator. It increases blood flow to the extremities. When a patient is prescribed cilostazol, it is important to know if they are taking other vasodilators, such as nitroglycerin or sildenafil (Viagra®).
Pentoxifylline and cilostazol help to reduce the pain of intermittent claudication. They are used for symptom management but do not cure PAD.
Surgical Interventions: Because medications do not cure PAD, advanced stages threatening limb loss require revascularization. This can include minimally invasive angioplasty and stenting, atherectomy (mechanically removing plaque), or peripheral artery bypass surgery to reroute blood around the blockage.
Can a Patient Have PAD and CAD?
Yes, and it is incredibly common. Because atherosclerosis is a systemic vascular disease, a patient who has plaque buildup in their legs (PAD) is at a significantly high risk of also having plaque buildup in their heart (CAD), and vice versa. Patients diagnosed with one condition should be aggressively screened and medically managed for the other.
Summary
Both CAD and PAD result from the dangerous systemic progression of atherosclerosis, decreasing vital arterial blood flow. While they share identical risk factors and fundamental pathophysiology, their distinct locations require targeted monitoring: CAD threatens the heart, while PAD threatens the extremities. By mastering the differences in their clinical presentation, such as angina versus claudication, nurses and healthcare providers can deliver rapid, highly effective guidance and treatment.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
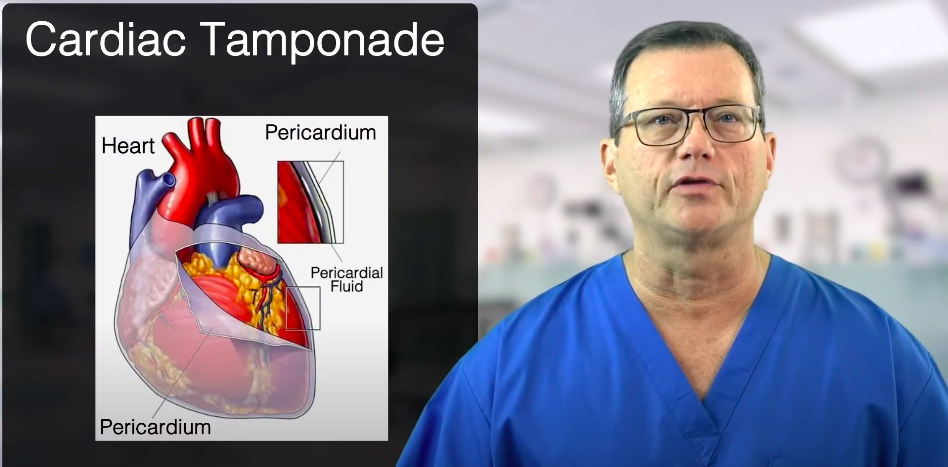
Understand the procedure for removing pericardial sac fluid in cardiac tamponade and the urgency of prompt intervention for this life-threatening condition.
Understand Hypovolemia, a condition marked by a decrease in blood volume due to fluid loss or bleeding, through our informative article.