VF and PVT: Care of the Patient with a Shockable Rhythm
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Table of Contents
- Defibrillation
- Rhythm-Based Management
- Ventricular Fibrillation
- Pulseless Ventricular Tachycardia
- Shocking the Patient
- Intravenous Access
- Other Access for Cardiac Arrest Drugs
- Epinephrine
- Airway Management
- Refractory Ventricular Fibrillation and Pulseless Ventricular Tachycardia
- Outcome
- Prognostication During CPR
- Summary
Article at a Glance
- Some patients with a shockable rhythm require components of BLS, ACLS, and post-cardiac arrest care.
- When using manual defibrillators, clinicians must clear the patient, stretcher, and equipment before delivering a shock. CPR is performed until it’s time to shock.
- Ventricular fibrillation and pulseless ventricular tachycardia are lethal rhythms requiring defibrillation as soon as possible after arrest.
- In ACLS, drugs may be given intravenously, intraosseously, through a central line, or through an endotracheal tube if the patient is intubated.

The cardiac arrest algorithm details general care for patients with shockable heart rhythms, such as ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT). VF is a disorganized and chaotic rhythm, while pVT represents an organized rhythm. Neither generates the blood flow required to sustain life, so they’re classified as lethal rhythms.1
There are three intervention groups: basic life support, advanced cardiac life support, and post-cardiac arrest care. Clinicians are successful if the patient receives early high-quality CPR and rapid defibrillation within minutes of collapse.
Other interventions are administration of intravenous epinephrine and airway management with advanced airways. They increase the rate of return of spontaneous circulation but not survival rates to hospital discharge.
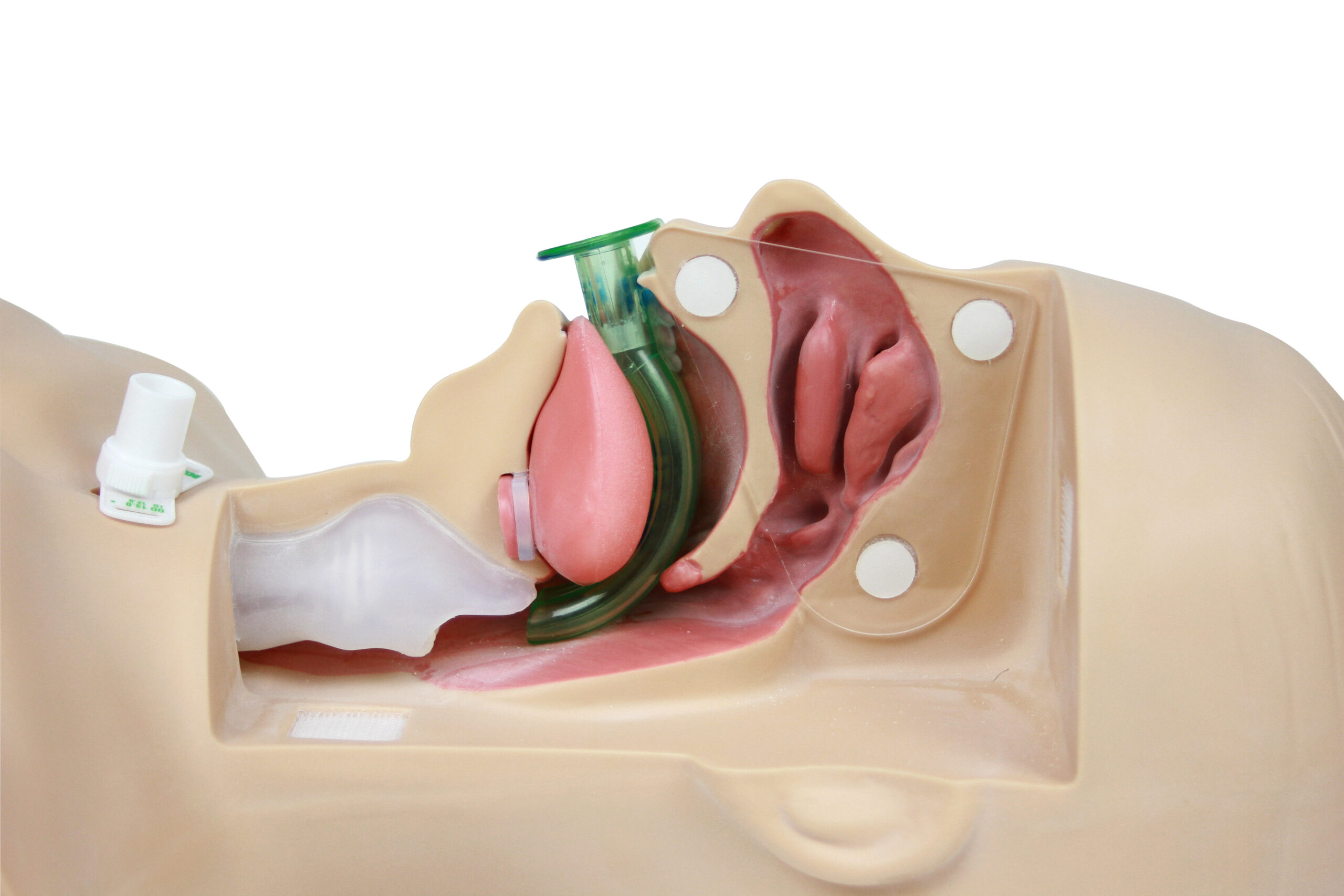
AHA algorithms have been simplified with a great emphasis on high-quality CPR. Clinicians must minimize chest compression interruptions. Interruptions are only necessary to assess rhythm, shock VF/pVT, perform a pulse check when an organized rhythm is detected, or place an advanced airway such as an endotracheal tube.
It’s recommended that clinicians monitor the patient’s physiologic parameters, which aid in assessing CPR quality. Parameters include partial pressure end-tidal CO2 (PETCO2) monitoring, arterial pressure monitoring during the relaxation phase of chest compressions, and central venous oxygen saturation (SCVO2) monitoring.
Defibrillation
In most cardiac arrests, the first provider immediately starts CPR with chest compressions while the second provider retrieves the defibrillator, attaches its pads to the patient, and checks the rhythm.2 The pads are placed directly on the skin at the anterior–lateral aspects of the chest.
Alternative positions include anterior–posterior, anterior–left infrascapular, and anterior–right infrascapular regions of the thorax.

Related Video – One Quick Question: Should You Choose CPR or Defibrillation?
The recommended defibrillator designs are biphasic truncated exponential (BTE) and rectilinear biphasic (RLB). They have different peak currents at the same energy settings. The energy outputs adjust based on the amount of patient impedance. RLB waveform defibrillators deliver more energy than the selected dose because energy is based on patient impedance. A 120 J dose delivers around 150 J.
Studies show BTE and RLB defibrillators are highly effective in converting shockable cardiac arrest rhythms, as emphasized in the adult cardiac arrest algorithm.3 The energy setting for the first shock is based on the manufacturer’s settings. First-shock success occurs when the rhythm terminates five seconds after shock delivery. The success rate is between 85% and 98% when the energy setting of both BTE and RLB is ≤200 J.

Rhythm-Based Management
Rhythm checks must be brief. Clinicians perform pulse and rhythm checks in 10 seconds or less. If the provider is not sure they can feel a pulse, they should immediately perform chest compressions.4
Ventricular Fibrillation
During VF, multiple areas in the ventricles chaotically depolarize and repolarize, causing a loss of pumping action to the heart. The ECG shows signs of voltage fluctuations. Coarser waves represent high-amplitude waves while fine waves represent smaller amplitudes.
In its early stages, VF has coarser amplitudes. Left untreated, these coarse waves transform into finer amplitude waves until the victim converts into asystole.
The heart rate during VF is very rapid and chaotic. The QRS complex cannot be appreciated, and the P wave is absent.

Related Video – ECG Rhythm Review: Ventricular Fibrillation
Read: Ultimate Guide to ACLS Algorithms: Cardiac Arrest
Pulseless Ventricular Tachycardia
During pVT, the heart rate is fast with a regular rhythm. The QRS complex is wide, and the P waves are absent. There are three or more beats of ventricular origin in a row. P waves are sometimes present, but they’re not related to the QRS complex.
Clinicians have difficulty differentiating ventricular tachycardia from supraventricular tachycardia with aberrant conduction. When in doubt, clinicians should assume the patient is in ventricular tachycardia.

Related Video – ECG Rhythm Review: Polymorphic VT (Torsades de Pointes)
Shocking the Patient
Once VF or pVT is confirmed (via AED or ECG monitor), providers deliver a shock. First, clinicians charge the device while continuing CPR. Once charged, it is imperative that providers “clear” the patient. Clinicians ensure there are no personnel touching the patient, the gurney, or any equipment attached to the patient before delivering the shock. For a broader explanation of the relationship between compressions and shocks, see defibrillation vs CPR.
Immediately following the shock, providers perform high-quality CPR for two minutes before checking for a pulse. First-shock success rates are high, though it depends on how long the patient has been down.
If the first shock fails, providers administer another shock after two minutes of CPR, following the defibrillator manufacturer’s instructions for shock dosage. Studies show a peak current of 150 J fixed BTE or RLB waveforms terminates persistent VF. There is no change in return of spontaneous circulation or survival to hospital discharge when a fixed dose is given versus an escalating dose.
If a provider uses a defibrillator that allows for energy dose adjustment, the provider may increase the dosage for the second and subsequent shocks.
The single-shock strategy with continued CPR for 2 minutes after administering the shock is preferred over the stacked-shock strategy.5
Intravenous Access
Epinephrine and other antiarrhythmic medications can facilitate a perfusing spontaneous rhythm.6 This includes agents such as amiodarone and lidocaine in ACLS. An intravenous cannula or intraosseous cannula can be used to rapidly deliver fluids and medications into the central circulation during CPR.
Clinicians should consider inserting an intravenous cannula after providing the first shock while minimizing interruptions in chest compressions. If intravenous access is not feasible, clinicians use intraosseous access. The medullary sinusoids of long bones are resistant to collapse and adequate for drug delivery to the central circulation.
When deciding to gain IV/IO access, remember: high-quality CPR supersedes defibrillation, and defibrillation supersedes establishing IV/IO access.
Other Access for Cardiac Arrest Drugs
If intravenous or intraosseous access cannot be established, the next step is central venous catheterization, which directly delivers the drug to the central circulation via the subclavian or internal jugular veins. Central lines are also used for physiologic monitoring (e.g., ScvO2, central pulse pressure) to assess CPR quality and predict ROSC.
Related Video – Understanding the Post Cardiac Arrest Algorithm
Central line placement may cause a prolonged interruption in chest compressions and is a relative contraindication for fibrinolytics if later needed.
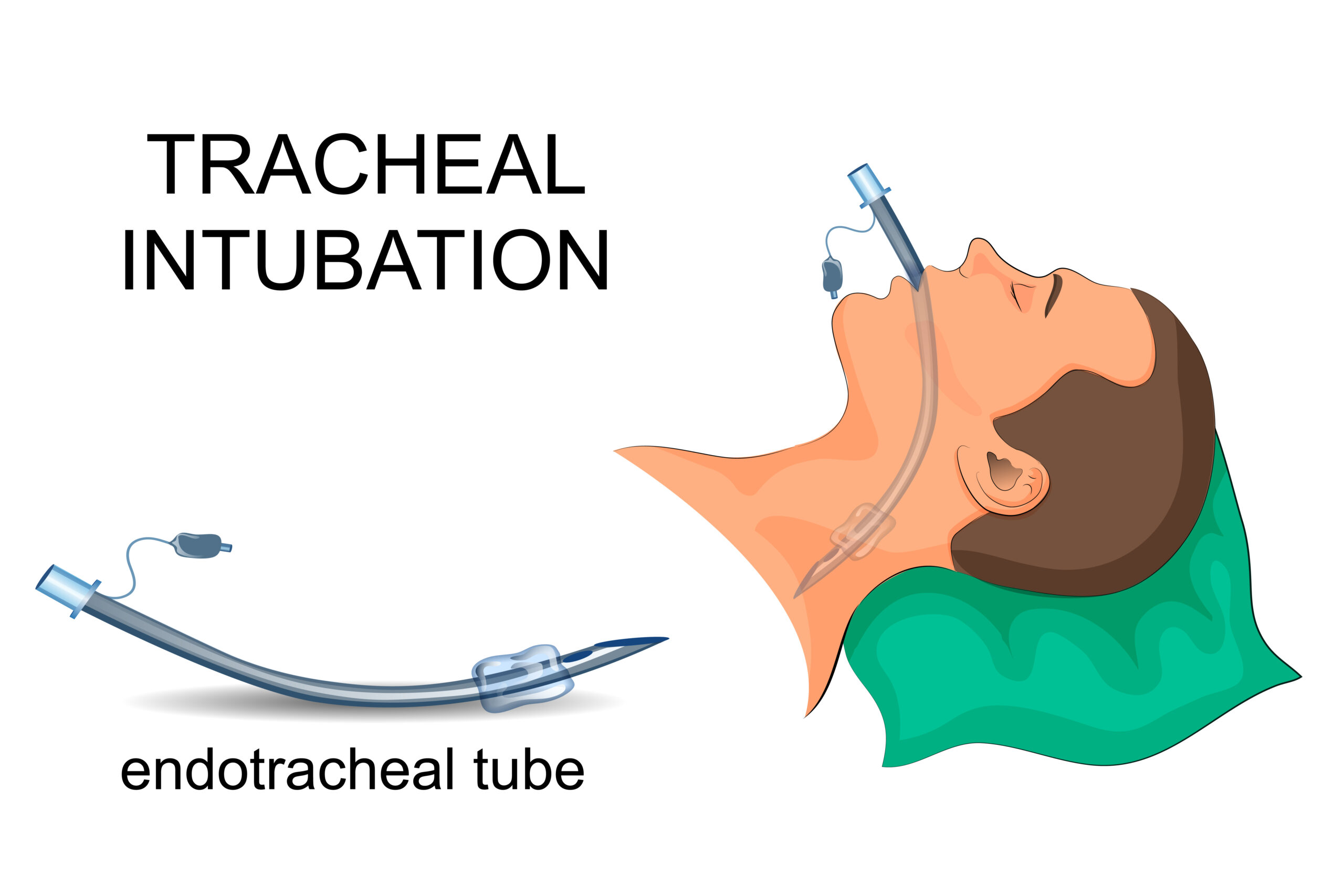
Absorption of drugs via an endotracheal tube is possible for naloxone, atropine in ACLS, vasopressin, epinephrine, and lidocaine (remember NAVEL). No studies have determined the absorption efficacy of amiodarone.7
Lower blood concentrations result via the endotracheal route compared to the intravenous route, potentially worsening hypotension and reducing the potential for ROSC. The dose of epinephrine via the endotracheal route must be 3–10× the IV dose, diluted in 5–10 mL normal saline and injected into the endotracheal tube.
Epinephrine
Epinephrine is an alpha-adrenergic drug that causes vasoconstriction. It increases coronary and cerebral perfusion pressure during CPR and is administered at a dose of 1 mg IV/IO every 3–5 minutes during cardiac arrest.8 High doses may increase myocardial workload and decrease subendocardial perfusion.
Follow IV boluses with a 20 mL saline flush and elevate the limb to facilitate delivery to the central circulation.
Airway Management
All patients needing CPR should receive positive-pressure ventilation via a bag-mask device with supplemental oxygen at 100% concentration. During the first minutes of witnessed cardiac arrest, arterial oxygen often remains adequate; chest compressions are the priority to circulate oxygen.

Related Video – Understanding Bag Valve Mask Usage During CPR
After the second shock, consider advanced airway placement. An advanced airway allows asynchronous ventilations without interrupting compressions. There is no clear advantage of endotracheal tube over bag-mask device; all providers must be proficient with bag-mask ventilation.
Refractory Ventricular Fibrillation and Pulseless Ventricular Tachycardia
After the third shock, administer amiodarone 300 mg IV/IO for refractory VF/pVT, followed by a 20 mL saline flush. If ineffective after the next shock and 2 minutes of CPR, a second dose of 150 mg may be given.9
Outcome
If the patient achieves ROSC, proceed to post-cardiac arrest care. If not, evaluate for reversible causes (Hs and Ts).
Prognostication During CPR
For intubated patients, use waveform capnography to monitor end-tidal CO2. Persistently low ETCO2 (<10 mm Hg) after ~20 minutes of high-quality CPR predicts poor outcome and should trigger troubleshooting for equipment or physiologic issues (e.g., tension pneumothorax).
Summary
For VF/pVT cardiac arrest, combine BLS, ACLS, and post-arrest care. Prioritize continuous high-quality CPR, rapid defibrillation, appropriate medications via IV/IO (or alternatives when necessary), and effective airway/ventilation strategies.
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
1. Mayo Clinic. Ventricular fibrillation. 2022.
2. American Red Cross. AED Steps. 2022.
3. Mark S. Link, Lauren C. Berkow, Peter J. Kudenchuk, Henry R. Halperin, Erik P. Hess, Vivek K. Moitra, Robert W. Neumar, Brian J. O’Neil, James H. Paxton, Scott M. Silvers, Roger D. White. Adult Advanced Cardiovascular Life Support. American Heart Association. 2015.
4. Mayo Clinic. Cardiopulmonary resuscitation (CPR): First aid. 2022.
5. American Heart Association. Management of Cardiac Arrest. 2005.
6. Andry Papastylianou and S. Mentzelopoulos. Current Pharmacological Advances in the Treatment of Cardiac Arrest. Emergency Medicine International. 2021.
7. Raehl CL. Endotracheal drug therapy in cardiopulmonary resuscitation. Clin Pharm. 1986
8. Jesse Borke, MD, FACEP, FAAEM; Chief Editor: Kirsten A Bechtel, MD. Cardiopulmonary Resuscitation (CPR). Medscape. 2021.
9. Jeffrey B. Florek; Daniel Girzadas. Amiodarone. National Library of Medicine. 2021.
More to Learn
Learn Managing Respiratory Arrest and Maintaining Airway Patency, including Oropharyngeal and Nasopharyngeal Airway Management in our detailed article and video illustrations.
PEA is often caused by medical conditions that cause reversible cardiac arrest. Download the PDF and read our detailed article on Treating Reversible Causes, ROSV, and Terminating Resuscitation Efforts.