Cardiac Output Fundamentals
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Cardiac output (CO) is the amount of blood ejected from the heart over one minute.
- The formula is CO = Heart rate X Stroke volume.
- The average CO is approximately 5 liters per minute.
- Included is an explanation of atrial kick, end-diastolic volume, end-systolic volume, ejection fraction, and Frank-Starling Law and how they relate to stroke volume and cardiac output.
- Key takeaway: Always treat the rate first.
Overview of Cardiac Output
What is cardiac output? Cardiac output is the amount of blood ejected out of the heart and into the cardiovascular system over one minute, a concept emphasized in pediatric emergencies and covered in PALS certification training. The cardiac output formula we use to calculate this measurement is:
Cardiac output = Heart rate × Stroke volume
Let’s take a look at that heart rate. It’s pretty simple. The heart rate is the number of beats per minute. For the purpose of this discussion, we are going to use a heart rate of about 70 beats per minute (bpm). If you go back look at the algorithms for treating heart rates, generally, they are pretty easy and quick to deploy.
In most adults at rest, normal cardiac output is roughly 5–6 liters per minute (it varies by body size and activity level).
Related Video – What is Cardiac Output?
Now, we get to stroke volume. The stroke volume is the amount of blood ejected by the ventricles with each contraction. On a given day, the average person has a stroke volume of about 70 mL. That’s for one beat.

An example calculation of cardiac output. An average cardiac output is about 4900 mL per minute or rounded to about 5 liters per minute.
Looking at this formula, if we take a heart rate of 70 bpm and a stroke volume of 70 mL, we are going to come up with a cardiac output of about 4900 mL. If you look at some of the texts, they say the average cardiac output is about 5 liters per minute. That’s where they got the number from because they are using averages. A person’s actual cardiac output will differ, but for the purpose of this discussion, we are going to use those averages.
Before we dive into stroke volume, let’s back up and take a closer look at the dynamics of blood flow through the heart. We were taught that blood enters the right atrium and then the right atrium contracts and squeezes blood into the ventricles. Those statements are about 20% true. Here’s why. As blood is coming in from the superior and inferior vena cava, it is entering the right atrium. Keep in mind that the tricuspid valve is between the atrium and the ventricle. The valve is like a one-way trapdoor. As long as the pressure is greater on the top, the valve is going to open and blood is going to flow through it. Read: Systems of Care: In-Hospital Cardiac Arrest In fact, the only time the one-way valve closes is during systole when the ventricles are contracting. The pressure becomes greater in the ventricles, and it slams those valves closed. The blood will either go through the pulmonary artery or out through the aortic valve and into the aorta if it is coming from the left ventricle. Therefore, all the blood coming into the right atrium actually passes right through the valve and starts filling up the ventricles, too.Review of Blood Flow Through the Heart
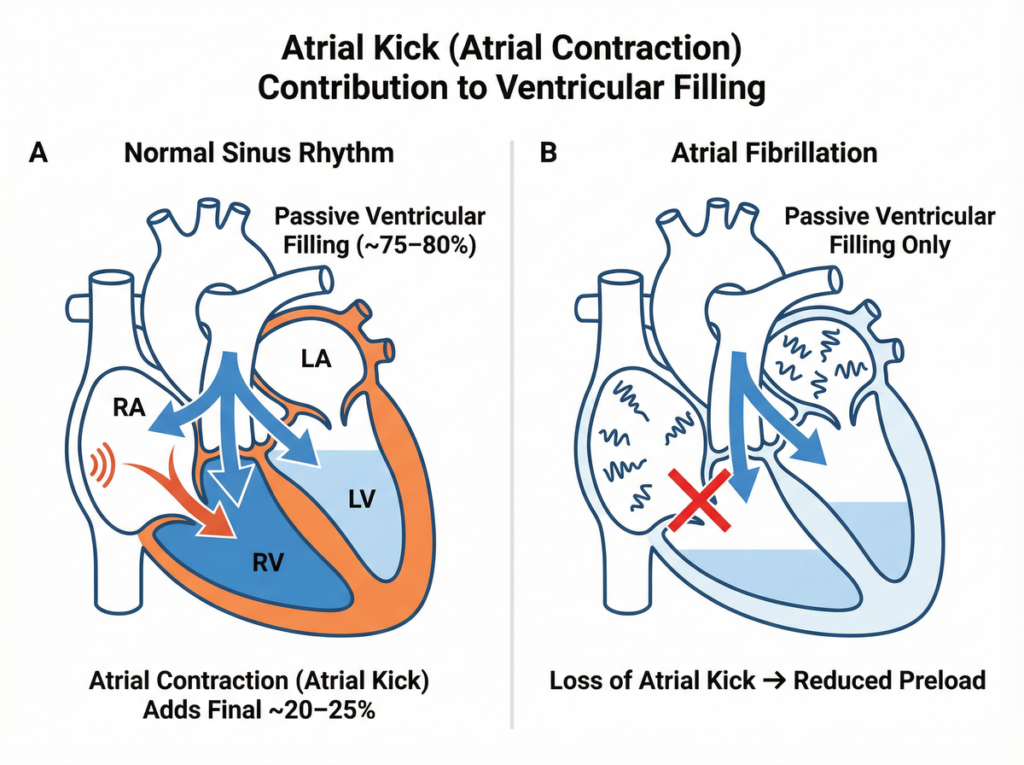
Blood comes from the superior vena cava and inferior vena cava. The blood enters the atrium, passes right through the valve, and starts filling up the ventricular chambers. The ventricle is getting more and more full of blood, and so is the atrial chamber. Then, the atrial chamber contracts and it squeezes its volume of blood into the ventricle. We called that volume the atrial kick. The atrial kick contributes about 20 to 25% of the additional volume reaching the ventricles. Essentially, it just tops off the tank. Atrial kick “tops off” ventricular filling in sinus rhythm (about 20–25%). In atrial fibrillation, this boost is lost, lowering preload and potentially cardiac output. Sometimes the atrial chambers contribute nothing. For example, with atrial fibrillation. Blood is coming into the atrial chamber, but the atrial chamber is just quivering. The blood goes into the ventricles, fills up the ventricles, but the atrial chamber never contracts because it is fibrillating. You lose maybe 25% of that blood that would have been injected into the ventricles. You lose your atrial kick because of the atrial fibrillation.Atrial Kick
End-diastolic Volume and End Systolic Volume
During diastole, blood is coming down and filling up the ventricular chamber. The blood is filling, filling, and filling…then, the atrial chamber contracts and kicks its volume into the ventricular chamber right before systole. The amount of volume in the ventricular chamber before the ventricles contract is called the end-diastolic volume.
The end-diastolic volume is more than the stroke volume. In this scenario, the end-diastolic volume would be around 120 mL. That 120mL is the volume of blood in the ventricle when it is completely full.
When systole occurs, the ventricle contracts and kicks out a stroke volume of about 70 mL. That leaves us with 50 mL leftover in the ventricular chamber. We call the blood that is left over the end-systolic volume, or the amount of blood that is left in the ventricular chamber at the end of systole.
Related Video – What is the Cardiac Cycle?

The end-diastolic volume is the total volume of blood in the ventricle right before systole.

During contraction, not all of the blood in the ventricles is pumped out. There is blood left over in the ventricle after contraction, which is known as the end-systolic volume.
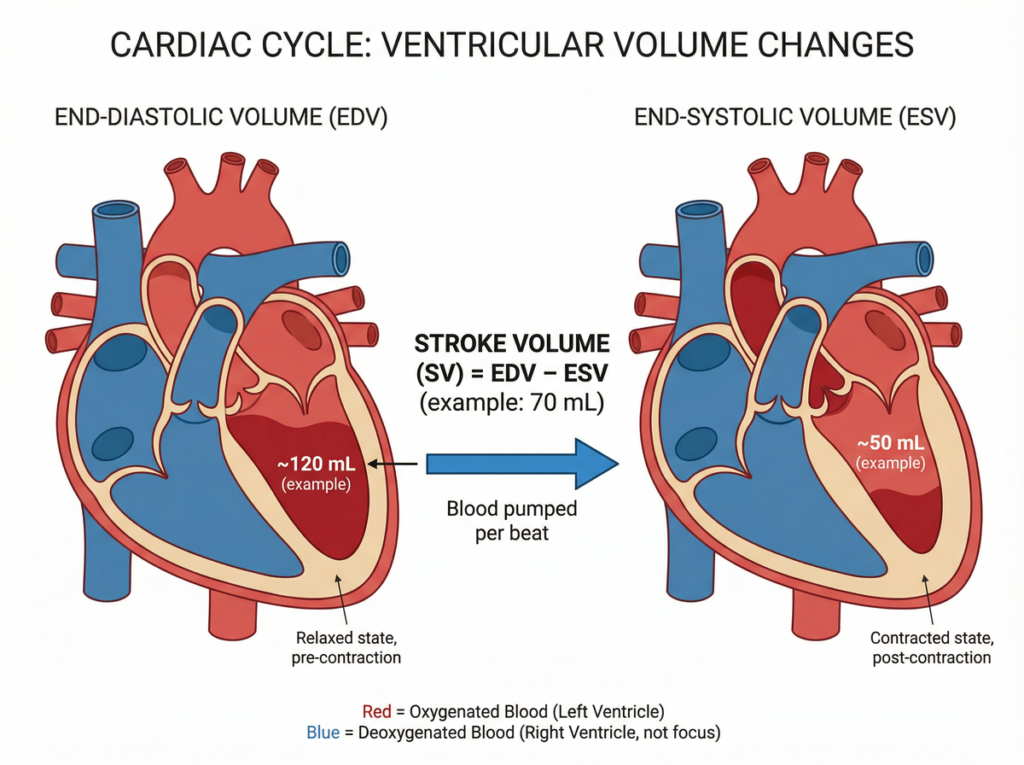
EDV is the volume in the ventricle right before contraction; ESV is what remains after contraction. Stroke volume equals EDV minus ESV.
Ejection Fraction
Stroke volume is the end diastolic volume minus the end systolic volume. The percentage of the stroke volume compared to the end diastolic volume is called the ejection fraction (EF). The ejection fraction is the percentage of blood that the ventricle pumps out with each contraction. For example, of that 120mL of blood in the ventricle when it’s full, we kicked out 70 mL. 70 mL divided by 120 mL is about 58%. The ejection fraction in this case is 58%.
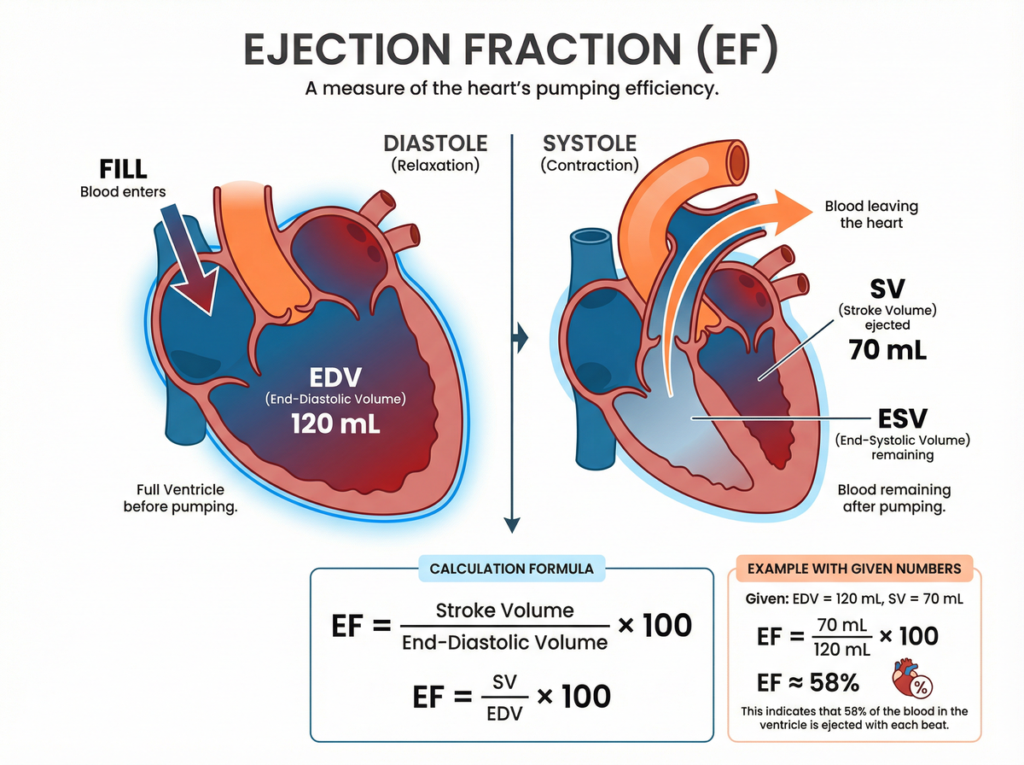
Ejection fraction is the percentage of blood ejected from the ventricle with each beat (EF = SV ÷ EDV × 100).
Related Video – What is Stroke Volume?
A normal ejection fraction is usually between 50 and 70%. On average, we like to see an ejection fraction above 60%. An ejection fraction less than 50% is a cause for alarm. Essentially, ejection fraction speaks to how well the heart is contracting. If it is less than 50% you need to wonder if it is it a systolic problem. Is there not good squeeze out of that ventricular chamber?
Related Video – What is Ejection Fraction?
Effect of Bradycardia and Tachycardia on Cardiac Output
Let’s look at the end diastolic volume and how it fits back into our cardiac output equation. If we have an extremely bradycardic patient with a very slow heart rate, that slow heart rate allows for adequate ventricular filling time. The patient will be getting a good end diastolic volume. In a bradycardic patient, the bradycardic heart rate probably won’t impact my stroke volume directly.
However, if you have an extremely tachycardic patient, the heart contracts before the blood can fill up the ventricular chamber adequately. The heart spits out less volume that it usually would. When airway control is required during resuscitation, confirm ET tube depth after securing the tube because changes in intrathoracic pressure from positive pressure ventilation can further alter preload and cardiac output; see ET tube placement depth for quick bedside checks. That’s why extremely tachycardic heart rates can directly impact your stroke volume. The heart just doesn’t have enough time for those ventricles to fill.
Now, take tachycardia and combine it with atrial fibrillation. Let’s say you have a patient in atrial fibrillation with a rapid ventricular response. Now the atrial kick is lost and there is reduced end diastolic filling time. Volume is lost from both atrial and ventricular chambers. That combination of heart conditions will directly reduce the cardiac output.
Factors Affecting Cardiac Output
Heart rate matters, but cardiac output is also strongly influenced by factors that change stroke volume and the heart’s ability to fill and eject blood. Common contributors include:
- Preload (ventricular filling): dehydration/bleeding lowers preload; intravenous fluids may increase preload.
- Afterload (resistance to ejection): elevated blood pressure or vascular resistance makes it harder for the ventricle to eject blood.
- Contractility: ischemia, cardiomyopathy, or myocarditis can reduce squeeze; inotropes can increase it in select settings. Structural abnormalities such as heart valve problems can also reduce forward flow and contribute to decreased cardiac output.
- Rhythm/AV synchrony: atrial fibrillation can reduce filling by eliminating the atrial kick.
- Valve disease: aortic stenosis or severe regurgitation can limit forward flow.
Frank-Starling Law
Another factor when considering cardiac output is called the Frank-Starling Law. The Frank-Starling Law says the greater the stretch of the myocardium, the greater the force of contraction. It’s easy to understand by using a balloon analogy. If you have a flat balloon with no volume in it, there’s no stretch and no contraction.
Now, let’s put a little volume into this balloon. It stretched a little bit, which means there is a little more strength of contraction. As more volume goes into the balloon there will be greater stretch.

To better understand the Frank-Starling law, think of the stretch of a balloon as an analogy to the stretch of the heart.
Let’s think back to our patient who has atrial fibrillation with rapid ventricular response. Since the patient had atrial fibrillation,you need to account for that by reducing the volume of the balloon. So, take a little volume out. If the patient is also tachycardic with reduced filling time, take even more volume out of the balloon.
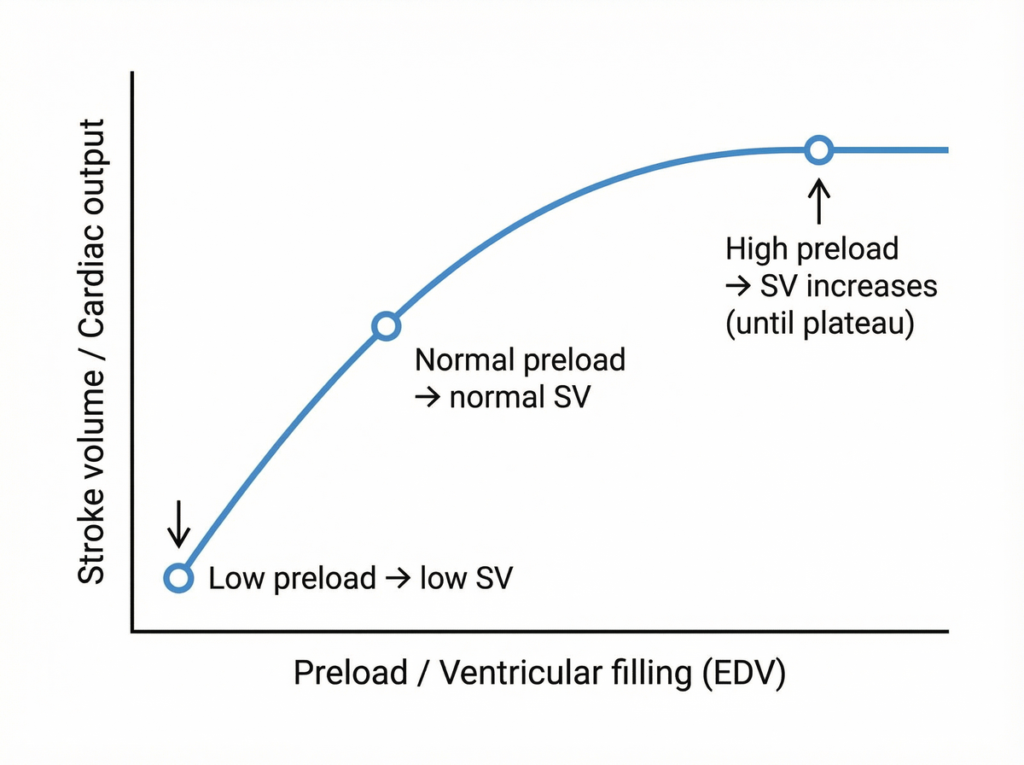
Frank–Starling Law: increasing ventricular filling (preload) increases stroke volume up to a physiologic plateau.
Now you can see the impact of Frank-Starling’s Law on a patient that has atrial fibrillation with rapid ventricular response. You’ve lost more volume coming into the heart, and now there is less stretch to the myocardium. Therefore, you’ll have less force of contraction and less cardiac output. That is Frank Starling’s Law very simplified.
Other Methods to Calculate Cardiac Output
In clinical settings, cardiac output can be estimated or measured using several methods. The choice depends on how accurate the team needs to be and how invasive the measurement can be.
Fick Principle (oxygen consumption method)
The Fick principle estimates cardiac output by comparing oxygen content in arterial blood to venous blood and relating that difference to the body’s oxygen consumption. It can be performed during right-heart catheterization and is often considered a highly accurate reference method when all variables are measured carefully.
Thermodilution (pulmonary artery catheter)
Thermodilution measures cardiac output by injecting a small amount of cool fluid and analyzing downstream temperature changes. This method is performed using a pulmonary artery catheter and is used in select critically ill patients when invasive monitoring is warranted.
Echocardiography (stroke volume estimation)
Transthoracic echocardiography can estimate stroke volume and cardiac output noninvasively. A common approach is to calculate stroke volume from left ventricular outflow tract (LVOT) measurements and then multiply by heart rate.
To review our formula, cardiac output equals heart rate times stroke volume. Say we’ve got a heart rate of 70 bpm and a stroke volume of 70 mL. If the patient becomes bradycardic and that heart rate drops to 35 bpm, my cardiac output is cut in half. Now, let’s say that the patient is extremely tachycardic. That directly reduces the stroke volume, which reduces the cardiac output. What is the takeaway from this segment? Always treat the rate first. Why? One, because it’s quick and easy. Go back and look at the treatment algorithms. You can give a drug, use pacing, or cardiovert them. It’s quick and easy, which is a good thing. For example, if I’m 40,000 feet in the aircraft and my patient starts to decompensate, I want a treatment that is quick and easy. Treat the rate first. So, always treat the rate first. Such as in bradycardia because the stroke volume might be fine, but it’s the rate that is impacting the cardiac output. In tachycardia, the rate is directly reducing the stroke volume, which is reducing their cardiac output.Summary

More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn

This article and video review Glomerulonephritis. Learn about the etiologies, nursing assessment, and interventions for...
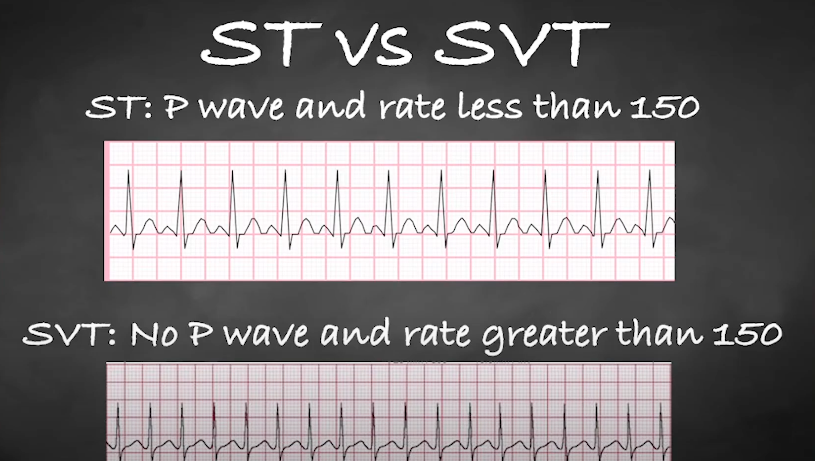
Understand the differences between ST and SVT during an electrocardiogram (ECG) interpretation by reading our comprehensive article.