ACLS Hs & Ts – Tension Pneumothorax
Designed for ACLS learners and clinical providers, this guide covers the pathophysiology, rapid identification, and emergency treatment of tension pneumothorax. By the end of this article, you will be equipped to recognize the clinical signs of this condition and immediately perform a life-saving needle decompression without waiting for imaging.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
Core Takeaway: Tension pneumothorax is a life-threatening emergency where air becomes trapped in the pleural space, compressing the lungs and vena cava; if suspected, it requires immediate needle decompression to restore cardiac output.
- Tension pneumothorax is one of the Hs and Ts and a reversible cause of cardiac arrest.
- It is caused by a hole in the lung, often due to PPV that allows air to escape into the thorax, compressing the vena cava and restricting blood return to the heart.
- The provider must know the signs and symptoms.
- Treatment is decompression of the pneumothorax using a needle into the chest, allowing air to escape.
- Within 15 seconds, the lung should expand, pulses should return, and the patient should improve.
Definition and Physiology of Tension Pneumothorax
A pneumothorax becomes a tension pneumothorax when air is trapped in the pleural space and cannot escape. A penetrating chest injury or internal lung tear can cause this. Essentially, air is leaving the lung and collecting in the pleural space.
Air is trapped in the pleural space during tension pneumothorax.
A hole in a lung sometimes creates a one-way valve. As air leaves the lung, it collects in the pleural space but cannot return. Pressure and tension build up. The tension pushes on all the lung structures towards the middle of the body. This is a severe problem because the vena cava lies in the middle of the body, returning blood to the heart.
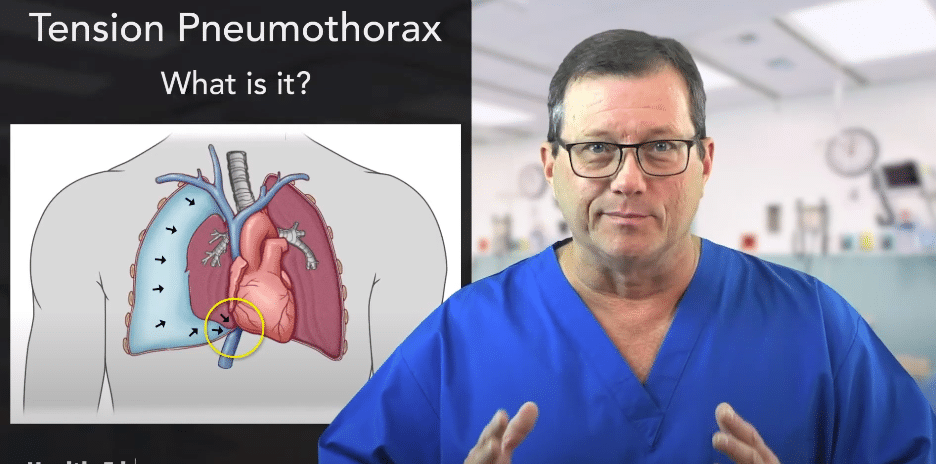
Air pressure pushes on the lungs and other organs. The vena cava is circled in yellow.
Remember, the pressure in the vena cava is very low. Right before the vena cava hits the heart, the blood pressure is around 5 mmHg. Keep in mind, there’s no delineation between systolic or diastolic at this point. The pressure pushing on the vena cava may completely compress it, obstructing the blood returning to the heart.
Fatalities from tension pneumothorax occur when the pressure builds up, compresses the vena cava, and blocks the blood returning to the heart. This obstruction often manifests as PEA ACLS, where electrical activity persists but no effective pulse is generated.
Signs and Symptoms
The following are key signs and symptoms of tension pneumothorax:
- Profound dyspnea: severe difficulty breathing
- Tachypnea: rapid breathing
- Hypotension: dropping blood pressure due to blocked venous return
- Absent breath sounds: typically unilateral (on one side)
- Jugular venous distention (JVD): visible bulging of the neck veins
- Tracheal deviation: shifting of the windpipe away from the affected side (note: this is a rare, late sign)
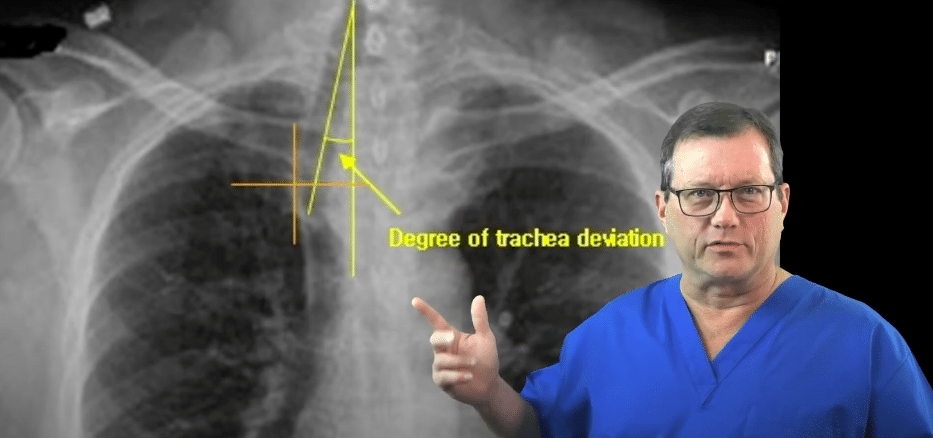
The trachea’s position shifts when a tracheal deviation is present.
Diagnosis
In an ACLS or emergency setting, tension pneumothorax is a purely clinical bedside diagnosis. If a tension pneumothorax is suspected based on the clinical signs (hypotension, JVD, and unilaterally absent breath sounds), you must not delay treatment to obtain an X-ray or other imaging.
Differential Diagnosis Note: Tension pneumothorax shares several features with cardiac tamponade, another critical cause of PEA (both cause severe hypotension and JVD). However, tension pneumothorax is distinguished by unilaterally absent breath sounds and hyperresonance to percussion on the affected side, whereas cardiac tamponade typically presents with muffled heart tones and equal, clear breath sounds.
Radiographic imaging, such as a chest X-ray or point-of-care ultrasound (POCUS), should only be used after initial stabilization and decompression to confirm the placement of interventions (like a chest tube) or to evaluate a stable, simple pneumothorax.
Treatment
To treat a tension pneumothorax, you must immediately decompress the chest. Creating an opening allows the trapped pressurized air to escape, relieving the compression on the vena cava and restoring blood flow.
Follow this sequence for needle decompression:
- Select Equipment: Use a large 3-inch, 12-gauge or 14-gauge needle/catheter.
- Find the Landmark: Start midclavicular at the clavicle and palpate down. The first rib you can appreciate is actually the second rib. From this rib, go down one space to find the third rib.
- Insert the Needle: Place the needle in the second intercostal space, aiming directly over the top of the third rib.
- Listen and Reassess: If the environment isn’t too noisy, you may hear the sound of air rushing out of the chest.
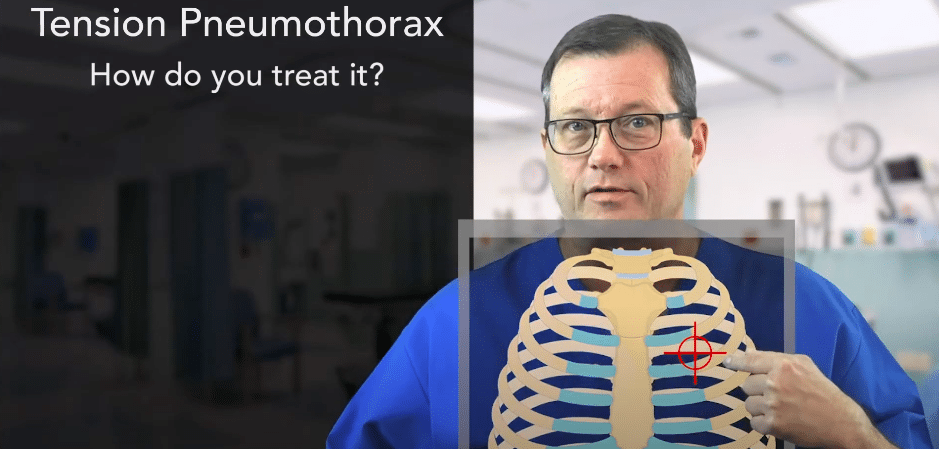
The insertion site for pleural decompression is midclavicular above the third rib.
You will often know the procedure was effective if the patient’s pulse quickly returns and compliance improves. While a pulse may return rapidly, results are not always instantaneous, and providers must continuously reassess. If the patient does not improve, the initial decompression may have been ineffective. At this stage, insert another needle half a centimeter to the right or left, but still over the third rib. It’s not uncommon to see patients with three or four needles placed to achieve adequate decompression.
Physicians may need to insert several needles into the patient.
Always ensure you are going over the top of the rib and not into the bone. You shouldn’t hit bone or feel resistance. Aiming over the top of the rib avoids the neurovascular bundle located on the bottom edge. Additionally, beware of the catheter kinking after insertion or failing to penetrate fully due to a thick chest wall (which is why a 3-inch needle is standard).
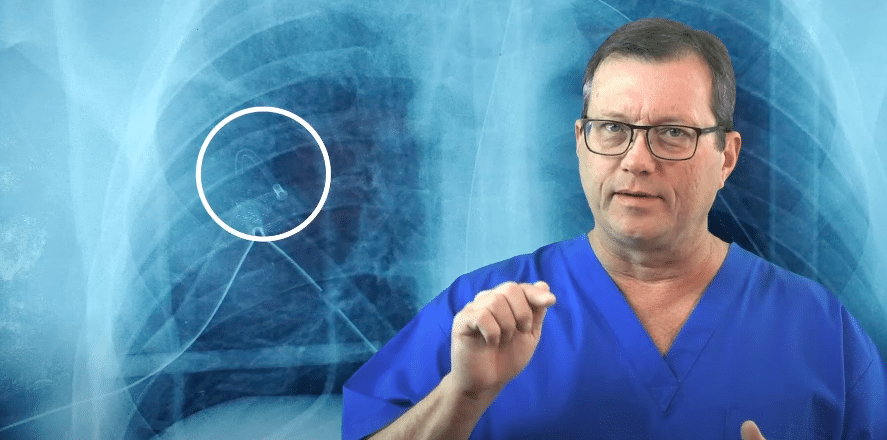
In this X-ray, the needle is kinked at the bone. Aim for the intercostal space, not the bone.
Read: Reversible Causes of Cardiac Arrest: Hs and Ts
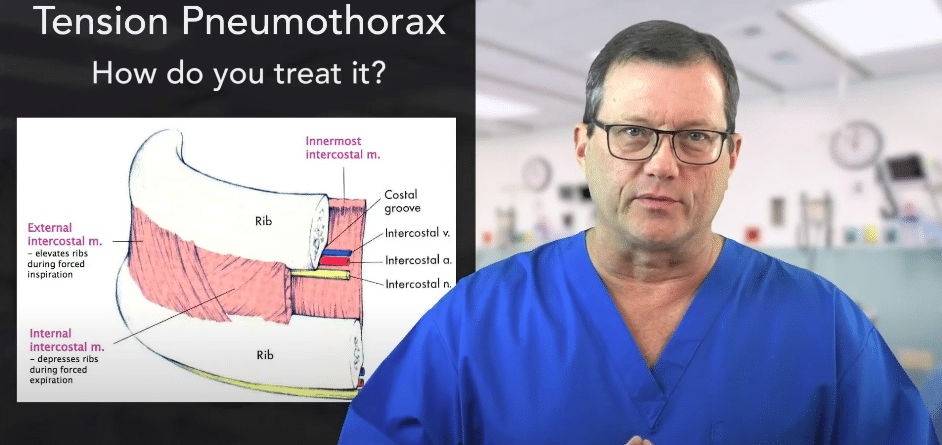
Physicians aim above the rib to treat tension pneumothorax, avoiding blood vessels and nerves.
To find pleural decompression landmarks, another avenue is to start at the sternomanubrial joint (angle of Louis) where the sternum meets the manubrium. Start here and navigate laterally to the midclavicular area. You should be right over the top of the third rib.
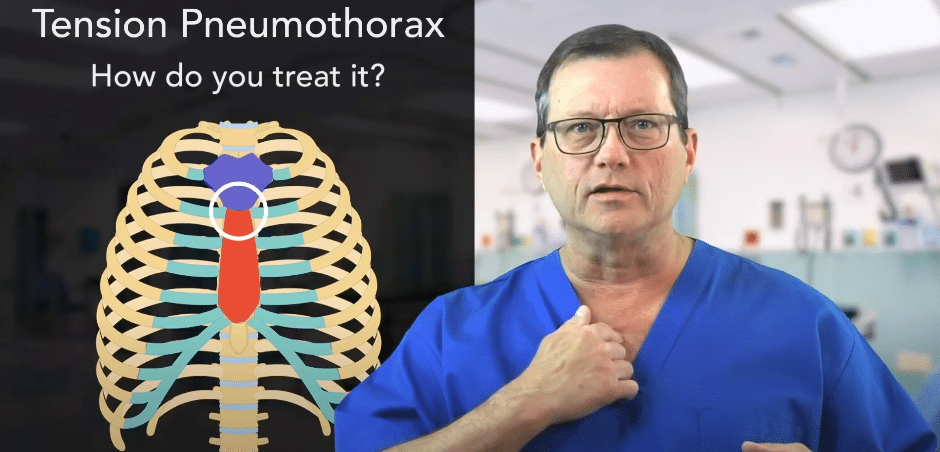
Another technique for locating the insertion site is to start at the sternomanubrial joint, which is marked by a white circle.
Who Does It Affect?
In a simple (spontaneous) pneumothorax, air leaks from the lung into the pleural space, but there is no one-way valve effect. The pressure equalizes rather than continually building up to dangerous tension levels. These patients tend to be tall, thin, high school-aged males.
By contrast, tension pneumothorax frequently occurs in patients receiving positive pressure ventilation (PPV). If your patient is intubated or being aggressively bagged, they are at a highly increased risk of developing a tension pneumothorax due to the forced air compounding the pressure leak.
For instance, a patient of mine in a helicopter developed a spontaneous tension pneumothorax right before we departed. All of a sudden, the high-pressure alarm went off on the ventilator. I took the patient off the ventilator and went to bag him, but I couldn’t get any air into him. I listened to his chest and determined the patient had absent lung sounds on one side.
We proceeded with immediate pleural decompression. I had a needle in my pocket, so I pulled it out, decompressed the patient, and after a few breaths, the patient became more compliant.
Summary
Tension pneumothorax is a critical emergency that occurs when air becomes trapped in the pleural space, building pressure that compresses the vena cava and blocks venous return to the heart. The classic signs include profound dyspnea, tachypnea, hypotension, unilaterally absent breath sounds, and jugular venous distention (JVD), with tracheal deviation appearing as a rare, late sign. Because this condition rapidly leads to cardiovascular collapse and PEA, it requires an immediate clinical diagnosis and rapid chest decompression with a 3-inch, 12-gauge needle above the third rib.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn

Read our detailed article and watch the video explaining Adaptive Support Ventilation. Learn the settings and review the advantages and...

Learn the 6 steps of BLS Assessment through the Systematic Approach to a Seriously Ill Patient. Read our detailed article on the mnemonic DRS. ABCD with video illustration.