Atropine in ACLS: A Comprehensive Guide to Mechanism, Dosing, and Indications
In the high-stakes environment of Advanced Cardiovascular Life Support (ACLS), Atropine serves as the primary pharmacological intervention for symptomatic bradycardia. This guide details how atropine modulates the heart’s electrical signals to increase beats per minute (bpm), outlines precise dosing guidelines, and identifies when to transition to transcutaneous pacing to improve patient outcomes.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Atropine is an anticholinergic/parasympathetic blocker that speeds up the heart rate.
- Atropine is indicated for symptomatic sinus bradycardia.
- The dose of atropine is 0.5 mg IV/IO every 3–5 minutes to a total dose of 3 mg.
- The provider should be prepared for transcutaneous pacing if atropine does not raise the heart rate.
Atropine’s Mechanism of Action and Physiological Effects
Atropine is an anticholinergic, also known as a parasympathetic blocker. Let’s review the sympathetic and parasympathetic nervous systems to better understand how atropine functions.
Atropine is an anticholinergic, also known as a parasympathetic blocker.
How does atropine affect the SA and AV nodes?
Atropine works by blocking the vagus nerve (parasympathetic influence). This action increases the firing rate of the Sinoatrial (SA) node and improves conduction velocity through the Atrioventricular (AV) node, effectively countering the “braking” action of the parasympathetic system.
Review of the Sympathetic and Parasympathetic Systems
The sympathetic nervous system is your “fight or flight” response. It speeds everything up. If the body were a car, the sympathetic nervous system would be the gas pedal. Conversely, the parasympathetic nervous system is the brake pedal, as it slows everything down. It’s the “rest and digest” system. Inside the body, both systems work simultaneously.
To visualize this “braking” mechanism, watch this brief overview of the parasympathetic system and how it regulates involuntary body functions.
If you want to speed up the car and increase the heart rate, you have a couple of options. One, you could simply press harder on the gas. In the case of Advanced Cardiovascular Life Support (ACLS), a hard press constitutes administering a sympathomimetic drug. Sympathomimetic drugs stimulate the sympathetic nervous system. Epinephrine is a great example. It directly stimulates the sympathetic nervous system.
Read: ACLS Drugs – Aspirin
Or you could take your foot off the brake a bit, which is what atropine does. Atropine is a parasympathetic blocker. By blocking the parasympathetic system, or “taking your foot off the brake”, you’re allowing the sympathetic system to dominate. Remember, the sympathetic nervous system actually increases the heart rate.
Atropine affects the parasympathetic system through its effects on the SA and AV node.
Conduction System of the Heart
Understanding atropine requires a firm grasp of how electrical impulses travel through the heart. The following videos break down the anatomy and physiology of this system.
First, we review the basics of heart conduction, tracing the impulse from the SA node to the Purkinje fibers.
Next, we explore what happens when primary pacemakers fail and how back-up pacemakers function within the conduction system.
Finally, we visualize how this electrical activity translates into waves and complexes on a monitor, explaining heart conduction in an ECG.
Atropine Indications
Atropine is the first-line drug for symptomatic sinus bradycardia, consistent with the ACLS bradycardia algorithm. It is also utilized in specific toxicology cases, such as organophosphate poisoning.
Atropine Dosing Guidelines
Bradycardia: The dosing of atropine is 1.0 mg administered IV/IO every 3–5 minutes. The maximum total dose is 3 mg.
Organophosphate Poisoning: You must administer significantly higher doses to reverse the toxin’s effects. The dosing is usually 2–4 mg (or higher) IV as a bolus, doubled every 5 minutes until pulmonary secretions dry up.
Atropine Contraindications and Adverse Effects
While lifesaving, atropine is not suitable for all patients.
- Ischemia: Use caution in the presence of acute coronary ischemia or myocardial infarction. Increasing the heart rate increases myocardial oxygen demand and can worsen ischemia.
- Heart Block: Atropine is generally ineffective for Mobitz II Second-Degree AV block or Third-Degree AV block with wide QRS complexes, as the block is often distal to the AV node.
- Adverse Effects: Common side effects include dry mouth, blurred vision, photophobia, urinary retention, and tachycardia.
Related Video – Atropine – Arrhythmia
Atropine may also be used to treat organophosphate poisonings. You must administer quite a bit of atropine to reverse the toxin’s effects. The dosing is usually 4–6 mg IV as a bolus.
Special Considerations
If you’re using atropine to raise the heart rate and it’s ineffective, you must transcutaneously pace the patient.
We must also ask why the patient is bradycardic. For example, a myocardial infarction may be present. In most people, the SA node receives its blood and oxygen supply from the right coronary artery. The right coronary artery also supplies the heart’s inferior wall. Therefore, it is not uncommon for bradycardia to be associated with an inferior wall myocardial infarction.
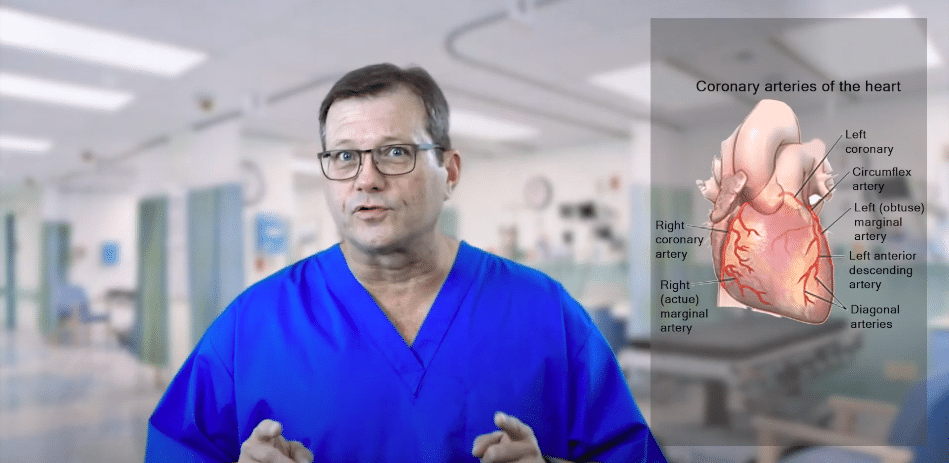
The right coronary artery supplies the SA node and inferior wall of the heart.
When should transcutaneous pacing be considered if atropine is ineffective?
If the patient remains symptomatic (hypotension, altered mental status, signs of shock) despite atropine administration, do not delay. You must transition immediately to transcutaneous pacing (TCP) or dopamine/epinephrine infusions.
Watch this demonstration on establishing transcutaneous pacing for a patient with unstable bradycardia.
Summary
Atropine is an anticholinergic, otherwise known as a parasympathetic blocker. It blocks the parasympathetic nervous system, allowing the sympathetic to dominate, thus raising the heart rate. It increases output from the SA node and conduction through the AV node. For a visual recap of the concepts discussed, including mechanism and indications, watch this summary on treating Arrhythmia with Atropine.
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
Endotracheal Intubation is a method of placing a tube into the windpipe (trachea). The process opens an airway and help the patient who can't breathe on their own.
Discover transcutaneous pacing, pad placement, and cardiac monitors at ACLS Certification Association. Our article enhances your knowledge of life-saving interventions.