What is Transcutaneous Pacing?
Transcutaneous pacing (also called TCP) is a temporary, non-invasive emergency intervention used to artificially stimulate the heart to contract by delivering electrical impulses through pads placed on the patient’s skin. It is typically deployed when a patient is suffering from hemodynamically unstable bradycardia that does not respond to pharmacological treatments.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Transcutaneous pacing is used during bradycardia when atropine is not effective, particularly in 2nd-degree Type II and 3rd-degree AV blocks.
- The placement of pads is the same as for defibrillation.
- The provider must know how to use the equipment at their facility.
- To use: change monitor to pacing mode, set the rate, and adjust the electrical current until there is a pacer spike on the monitor.
- Always check for a central pulse during pacing.
- The provider should consider sedation before pacing.
We use transcutaneous cardiac pacing on bradycardic patients when atropine in ACLS is ineffective, which typically occurs in lower blocks. Clinicians typically administer atropine for sinus bradycardia, sinus with a first-degree heart block, and sinus with a second-degree heart block Type 1 Wenckebach. Atropine can be effective for these blocks. If the block is below those levels, atropine will likely be ineffective. If a patient is experiencing a second-degree heart block (specifically Type 2) or a third-degree complete heart block, quickly prepare your pacer. In pediatric patients, bradycardia with poor perfusion is addressed in the PALS bradycardia algorithm, while adults are managed using the ACLS bradycardia algorithm. Since atropine does not work well for lower heart blocks, turn to transcutaneous pacing.A Quick Review on Transcutaneous Cardiac Pacing
Pad Placement
Before placing pads, ensure the patient’s skin is clean, dry, and free of excessive hair to reduce impedance and ensure good electrical contact. For transcutaneous pacing, you generally place the pads on the patient’s chest and back. This method is called anterior-posterior (AP) placement and is typically preferred for pacing because it “sandwiches” the heart, optimizing the current flow directly through the ventricles.
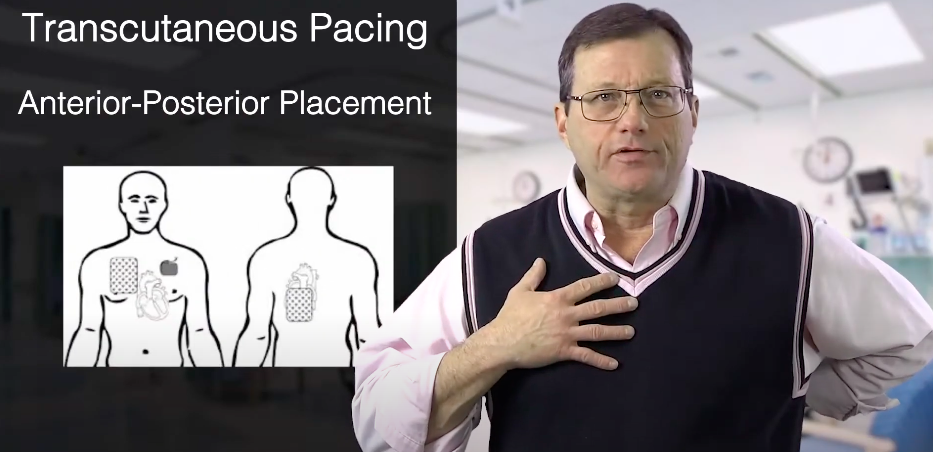
Anterior-posterior pad placement
After applying the pads, make sure the wires are not under the pads. Also, ensure there is no jewelry, medication patches, implanted devices, or anything else underneath the pads or in the way. You need a clear path from one pad, through the heart, to the other pad.
You may also place the pads anterolaterally (high right and low left of the chest, similar to standard defibrillation placement) if AP placement is impossible due to patient positioning or severe trauma. Regardless of the method, the goal is a direct path of electrical current through the heart.

Make sure there are no items under the pads or between the pads.
Read: What is Synchronized Cardioversion?
Cardiac Monitors
While there are some differences, most cardiac monitors operate similarly. You must know how your specific equipment works to initiate ECG pacing smoothly.
Cardiac monitors may look different but work the same.
Follow this general step-by-step workflow:
- Set the Mode: Turn the monitor to “Pacing” mode. Most standard protocols recommend starting in Demand mode (synchronous) so the pacer only fires when the patient’s intrinsic rate drops below the set limit, but always follow your local protocol.
- Set the Rate: Follow your local protocols to set the pacing rate. A standard starting pace is typically 60 to 80 ppm (paces per minute).
- Adjust the Energy (Milliamps/mA): Slowly turn up the current (mA) on the dial starting from zero.
- Achieve Electrical Capture: Continue turning up the mA until you see a pacer spike immediately followed by a wide QRS complex and broad T wave.
- Confirm Mechanical Capture: Check for a corresponding pulse to ensure the heart is actually pumping blood.
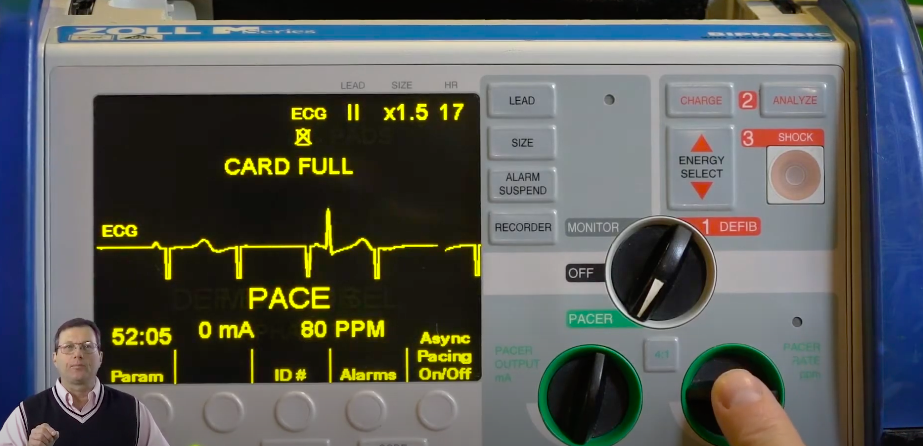
The provider is setting the pacer rate to 80 ppm, and there are currently 0 milliamps.
Electrical capture means the monitor shows the heart’s electrical system is responding to the shock (a spike followed by a QRS). Mechanical capture means the heart muscle is actually contracting and creating a pulse. Do not be fooled by false electrical capture (electrical artifact from the pads mimicking a QRS); you must always verify mechanical capture.
While pacing, feel for a femoral pulse. You should feel a pulsation coming off of the heart and down through the aorta. Remember, when you check for a pulse, check for a central pulse (femoral or carotid). It’s not uncommon for a patient to twitch severely while you’re pacing, so it may be hard to detect a pulse on the periphery. If palpation is difficult due to patient movement, instrument-based confirmation methods—such as looking for a matching pulse wave on a pulse oximeter (SpO2 plethysmograph) or using Doppler ultrasound—can be very helpful.
Troubleshooting Failure to Capture
If you reach high mA levels without capturing, consider the following:
- Pad Contact: Re-evaluate pad adhesion. Sweaty, hairy, or wet skin drastically increases impedance.
- Pad Placement: Ensure optimal AP placement to direct current precisely through the ventricles.
- Underlying Factors: Severe hypoxia, acidosis, or myocardial ischemia can significantly raise the pacing threshold, making the heart resistant to electrical stimulation.
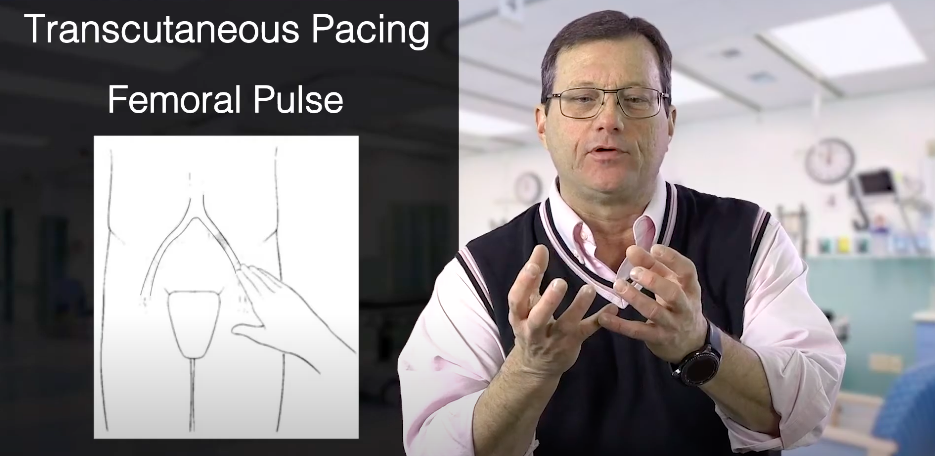
While pacing, find the femoral pulse.
Other Considerations
We want to use the least amount of energy necessary to generate a pulse. If the monitor’s milliamps are high, you may want to throttle back and use the least amount of energy necessary to generate a pulse.
Also, keep in mind that transcutaneous pacing hurts. You’re electrifying the body to get the heart to beat. Fentanyl might be a nice option because it doesn’t have a lot of hemodynamic effects. Importantly, you have to treat the pain. Your protocol may call for a little midazolam (Versed) or a sedative, which is appropriate.
Complications and Limitations of Transcutaneous Pacing
While lifesaving, TCP is a temporary bridge, not a permanent fix. Prolonged cardiac pacing can lead to skin burns and significant patient discomfort from skeletal muscle contraction. Because it requires passing electricity through the chest wall, patients with larger body habitus or severe barrel-chests (COPD) may have higher electrical impedance, making it extremely difficult to achieve electrical capture.
Contraindications and Cautions of Transcutaneous Pacing
Transcutaneous pacing is strongly contraindicated in cases of severe hypothermia, as the cold myocardium is highly irritable and pacing can easily trigger ventricular fibrillation (VF). It is also ineffective and not indicated for treating asystole. Extreme caution must be used if the patient has a transdermal medication patch in the pacing path (which must be removed and the skin wiped clean) or an implanted permanent pacemaker or defibrillator (pads should be placed at least 1 inch away from the device generator).
Summary
Transcutaneous pacing is the critical next step for hemodynamically unstable bradycardia when atropine is ineffective or contraindicated. Success depends on proper pad placement, achieving simultaneous electrical and mechanical capture, and aggressively managing the patient’s pain. Because TCP is strictly a temporary stabilization measure, providers must prepare immediately to bridge the patient to a more definitive treatment, such as transvenous pacing or expert cardiological intervention.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
Chest pain is a common symptom of ACS. Download the PDF and read the article to learn about the symptoms of ischemic chest discomfort and The STEMI Chain of Survival.

Use the Tachycardia with a Pulse algorithm and detailed article to learn how to appropriately assess and treat this patient.