Rhythm-based Management of Shockable and Non-Shockable Rhythms in Cardiac Arrest
Effective cardiac arrest management hinges on the clinician’s ability to rapidly differentiate between shockable and non-shockable rhythms. This guide explores the critical interventions for Ventricular Fibrillation (VF) and Pulseless Ventricular Tachycardia (pVT), the role of defibrillation, and the drug therapies essential for non-shockable conditions like PEA and Asystole.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Clinicians should be able to readily recognize the four rhythms associated with cardiac arrest: ventricular fibrillation, pulseless ventricular tachycardia, pulseless electrical activity, and asystole.
- Clinicians must minimize any interruptions in CPR when treating a patient with cardiac arrest rhythms.
- Administering electrical therapy as early as possible to patients with shockable rhythms increases the rate of successful return of spontaneous circulation.
- Clinicians should treat nonshockable rhythms with CPR and the drug epinephrine, which improves blood flow to the heart and brain.
Sudden cardiac arrest (SCA) features four electrocardiographic rhythms of interest, including (1) ventricular fibrillation (VF), (2) pulseless ventricular tachycardia (pVT), (3) pulseless electrical activity (PEA), and (4) asystole. Accurate rhythm recognition often goes hand-in-hand with understanding blood gas status, which is explained in detail in our guide on how to read arterial blood gases.
These electrocardiographic rhythms do not produce sufficient blood flow to sustain perfusion. VF is characterized by disorganized electrical activity, while pVT produces organized electrical activity.
Likewise, PEA is an organized electrical rhythm lacking sufficient mechanical ventricular activity to produce a detectable pulse.
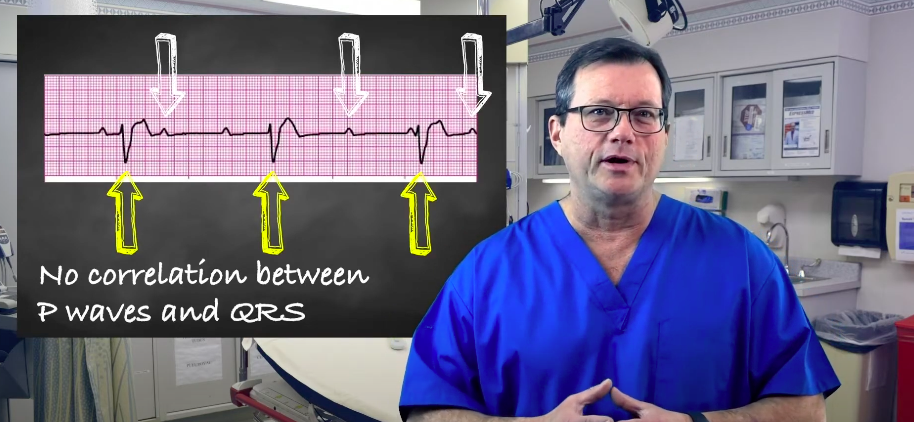
Asystole is an absence of ventricular electrical activity with or without atrial electrical activity, typically presenting as a flat line on the monitor; when atrial activity is present or suspected, consult the atrial rhythms guide to help interpret subtle atrial signals and avoid misclassification.
Survival rates and overall chances of survival decrease if there is a delay in defibrillation, especially for patients with shockable rhythms (VF and pVT).1 It is paramount for healthcare institutions to institute policies reducing the time to diagnose cardiac arrest and deliver rapid defibrillation. Fewer interruptions in chest compression also improve outcomes.
A clinician’s cardiopulmonary resuscitation (CPR) interruptions should be as brief as possible; the clinician should stop only to assess the rhythm, shock VF or pulseless VT, perform a pulse check when an organized rhythm is achieved, or to place an advanced airway. Intravenous or intraosseous access to drugs and fluids can be achieved without stopping CPR.
The clinician’s execution of rhythm-based management determines the patient outcome in cardiac arrest.
In reality, there are many more unsuccessful resuscitative efforts than successful ones, posing a question: are clinicians really managing their patients properly?
Shockable vs Non-Shockable Rhythms
Cardiac arrest rhythms are categorized into two groups based on their response to electrical therapy, commonly evaluated as shockable vs non shockable rhythms.
Shockable Rhythms (VF and pVT): These rhythms are caused by chaotic or rapid electrical signals and activity that prevents the heart from pumping. Defibrillation is effective here because the electrical shock depolarizes the entire myocardium simultaneously, essentially “resetting” the heart’s electrical system to allow the natural pacemaker to take over.
Non-Shockable Rhythms (PEA and Asystole): In these rhythms, the issue is not chaotic electricity but rather a lack of mechanical response or total electrical silence. Shocking these rhythms is ineffective because there is no chaotic electrical wave to reset; treatment relies on high-quality CPR and epinephrine to restore blood flow and electrical activity.
A patient’s arrest rhythms can change during advanced cardiac life support (ACLS). Interventions are adjusted based on the cardiac monitor’s rhythm, and these scenarios can be practiced in an ACLS simulator. Early in its progression, ventricular fibrillation features coarse waveforms that become finer if the clinician does not intervene or if poor technique is used. Eventually, fine VF becomes asystole. Early defibrillation is necessary for VF because, once it deteriorates into asystole, the treatment options are limited to CPR with medications, as outlined in the adult cardiac arrest algorithm. Asystole is a nonshockable rhythm.2 Alternatively, a clinician’s effective ACLS strategies can “improve” nonshockable rhythms such as PEA and asystole into VF and pVT, which can then be treated with electrical therapy. Healthcare clinicians should be ready to shock at any time.Change in Rhythms During ACLS
Defibrillators
Defibrillators are critical tools in ACLS, available in various forms including Automated External Defibrillators (AEDs), manual defibrillators, and Implantable Cardioverter-Defibrillators (ICDs).
Monophasic vs. Biphasic:
- Monophasic: Delivers energy in one direction. High energy (360 J) is required to be effective.
- Biphasic: Delivers current in two directions. This is more efficient, achieving the same efficacy with lower energy (120–200 J), which causes less myocardial damage.
Multimodal defibrillators in manual mode reduce interruptions in CPR, though user interpretation is required.

Defibrillators deliver electrical shocks to restore the heart rhythm.
How to Use an Automated External Defibrillator (AED) Safely
In the prehospital setting, AEDs are lifesaving tools that guide rescuers through the process. In this video, we review how to use an AED safely, from pad placement to how to safely deliver a shock while ensuring the patient is “clear.”
Shocking VF and pVT
The key to managing shockable rhythms is rapid defibrillation. High-quality CPR should be performed while the defibrillator charges, with interruptions only for the shock itself.
Deciding between immediate CPR or immediate defibrillation depends on the scenario. In this quick overview, we discuss choosing CPR or Defibrillation based on witnessing the arrest and the phase of resuscitation.
ECG Rhythm Review – Ventricular Fibrillation
Ventricular Fibrillation (VF) appears as a chaotic, quivering line with no discernible P waves, QRS complexes, or T waves. The waveform can be “coarse” (large amplitude) or “fine” (low amplitude). Watch this video to identify Ventricular Fibrillation on an ECG strip.

Ventricular Fibrillation
ECG Rhythm Review – Polymorphic Ventricular Tachycardia (Torsades de Pointes)
Polymorphic VT, or Torsades de Pointes, presents as a rapid rhythm (often exceeding 150 beats per minute (bpm)) where the QRS complexes appear to “twist” around the isoelectric line, changing amplitude and shape. This video reviews the unique characteristics of the ECG Rhythm of Polymorphic Ventricular Tachycardia (pVT).

Pulseless Ventricular Tachycardia
Drug Therapy in VF and pVT
While defibrillation is the priority, drug therapy plays a supportive role. Epinephrine is the primary vasopressor used to improve myocardial perfusion pressure during CPR.
The clinician administers epinephrine after the second shock attempt while CPR is in progress.

Epinephrine 1 mg/10 mL syringe
Epinephrine – ACLS Drugs
Understanding the dosing and timing of epinephrine is vital for ACLS success. This video details the pharmacology and administration protocols for Epinephrine in ACLS.
PEA and asystole are NONSHOCKABLE rhythms. The clinician administers epinephrine as soon as PEA or asystole is recognized and again every 3–5 minutes.5 Epinephrine is given via an intravenous bolus, followed by a normal saline flush. Epinephrine increases myocardial and cerebral blood flow during CPR. High-quality CPR and early epinephrine are the interventions of choice. The clinician performs intermittent pulse and rhythm checks every five CPR cycles (or approximately two minutes). This cycle continues until the patient develops a shockable rhythm or a definite pulse is felt. If a patient’s pulse is present after five CPR cycles, post-cardiac arrest care is started. If CPR is ineffective, the clinician must review possible reversible causes (see Hs and Ts) of PEA or asystole and treat them promptly. For example, in the case of hypoxemia, the clinician should prioritize advanced airway placement. In patients with volume loss or sepsis, intravenous or intraosseous administration of crystalloid fluids will benefit the patient; when a patient has had significant blood loss, blood transfusion is necessary. Clinicians should consider fibrinolytic therapy in patients who are believed to have experienced cardiac arrest as a result of a pulmonary embolism or a myocardial infarction caused by underlying heart disease. Needle decompression should be performed in patients with tension pneumothorax. The rescuer must diagnose and treat a patient’s cardiac arrest according to their cardiac rhythm. Shockable rhythms include VF and pVT, and the clinician should defibrillate as quickly as possible following diagnosis. Nonshockable rhythms include PEA and asystole, and the clinician should begin CPR and administer epinephrine as soon as possible.Nonshockable Cardiac Arrest Rhythms
Related Video – Introduction to the Hs and T
There are four rhythms associated with cardiac arrest: ventricular fibrillation, pulseless ventricular tachycardia, pulseless electrical activity, and asystole. It is imperative a clinician identify which of these rhythms is present before continuing care. High-quality CPR is not delayed, however, while the clinician gets information about the patient’s rhythm. Shockable rhythms are treated with electrical therapy as early as possible, while patients with nonshockable rhythms are treated with epinephrine and CPR until the patient has a return of spontaneous circulation or develops a shockable rhythm.Conclusion
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
1. M Holmberg, S Holmberg, J Herlitz. Incidence, duration and survival of ventricular fibrillation in out-of-hospital cardiac arrest patients in Sweden. Resuscitation. 2000.
2. American Heart Association. Management of Cardiac Arrest. 2005.
3. Jesse Borke, MD, FACEP, FAAEM; Chief Editor: Kirsten A Bechtel, MD. Cardiopulmonary Resuscitation (CPR). Medscape. 2021.
4. Callaway CW. Epinephrine for cardiac arrest. Curr Opin Cardiol. 2013.
5. Tony I. Oliver; Usama Sadiq; Shamai A. Grossman. Pulseless Electrical Activity. National Library of Medicine. 2022.
6. McGuff Medical Products. Epinephrine. 2021.
More to Learn
Understand the differences between CPR and defibrillation by reading our article. Learn about their critical roles in cardiopulmonary resuscitation and life-saving interventions.
Explore third-degree complete heart block and its ECG strip interpretation in our article. Gain insights into diagnosing and understanding this cardiac condition.