Acute Coronary Syndrome and Chest Pain
This guide provides a comprehensive breakdown of the ACLS Acute Coronary Syndrome (ACS) and chest pain algorithm. Designed for healthcare providers, EMS personnel, and ACLS learners, this article will teach you how to recognize ischemic symptoms, initiate early treatments, and apply the algorithm step-by-step to differentiate and manage a STEMI versus other acute cardiac events.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Chest pain, exhibited via retrosternal chest pressure or tightness, is a common ACS symptom.
- Ischemic chest pain may radiate to the jaw, arm, shoulder, and back.
- Practitioners should be aware of the differential diagnoses for chest pain.
- The STEMI Chain of Survival informs responders how to appropriately respond to a patient experiencing chest pain.
- Emergency dispatchers are often the first point of contact for ACS patients and play an important role in the STEMI Chain of Survival.
Identification of Chest Discomfort Suggestive of Ischemia
The Acute Coronary Syndromes Algorithm provides a structured clinical pathway to rapidly evaluate and manage patients experiencing ischemic chest pain. You can download the PDF flowchart below to keep as a quick clinical reference or study guide, but we will break down the exact sequence of steps immediately following the image.

Acute Coronary Syndromes Algorithm
Step-by-Step Algorithm Walkthrough:
- Symptom Onset: The algorithm begins when a patient experiences chest discomfort suggestive of ischemia. EMS is dispatched.
- EMS Assessment and Care: Pre-hospital providers administer the initial treatment bundle (Oxygen if indicated, Aspirin, Nitroglycerin, Morphine if needed) and obtain a pre-hospital 12-lead ECG. They provide early hospital notification if a STEMI is identified.
- ED Assessment (<10 Mins): Upon arrival, the ED rapidly assesses vital signs, establishes IV access, draws cardiac marker labs, and performs a focused physical and neurological exam.
- The Decision Point (ECG Analysis): The 12-lead ECG is reviewed by a physician. The rhythm is classified into one of three branches:
- STEMI: ST-segment elevation is present. The patient is rushed to the cath lab for reperfusion (PCI) or considered for fibrinolytics.
- NSTE-ACS: ST depression or dynamic T-wave inversion. High-risk patients may still go to the cath lab; others are admitted for monitoring and medical therapy.
- Low/Intermediate Risk ACS: Normal or non-diagnostic ECG. Patients are monitored, and cardiac markers are repeated to rule out infarction.
To fully grasp how these decision points branch based on the ECG interpretation, watch our visual breakdown in Understanding the Acute Coronary Syndrome Algorithm. You can also view our Acute Coronary Syndrome: ACLS Algorithm lesson for a deeper clinical overview.
Ischemic Chest Discomfort Symptoms
Chest pain is a symptom of ACS.1 Patients will complain of retrosternal chest discomfort. Pressure or chest tightness is a common symptom. Pain may radiate to the shoulders, neck, arms and jaw, while chest discomfort is sometimes present between the shoulder blades.
Patients may also complain of light-headedness, dizziness, syncope (fainting or passing out) or near syncope, diaphoresis (excessive, unprovoked sweating), or vomiting. A significant finding is sudden shortness of breath with or without chest discomfort. In many ACS cases, clinicians also administer key ACLS drugs to stabilize the patient. Understanding the benefit of morphine for acute coronary syndrome helps providers relieve chest pain and reduce sympathetic drive during ischemia.
Symptom Recognition Triggers the Pathway
It is vital to understand that recognizing these symptoms is only what triggers the algorithm pathway. Symptoms alone cannot diagnose a heart attack; only the 12-lead ECG classification can determine whether the patient is placed into the STEMI branch or the non-ST elevation branch.
While assessing symptoms, providers must rule out common differential diagnoses, which include aortic dissection, acute pulmonary embolism, acute pericardial effusion with tamponade, and tension pneumothorax. Caution: Differentials are clinically important because anchoring on an ACS diagnosis too early, and administering blood thinners like Aspirin, can be lethal if the patient is actually experiencing an aortic dissection.

Chest pain is a common symptom of acute coronary syndrome.
Read: Acute Coronary Syndrome: Emergency Medical Services
STEMI Chain of Survival
Why is rapid ACS intervention important? Every minute a coronary artery remains blocked, heart muscle tissue dies irreversibly. Rapid intervention is entirely time-based; meeting strict “door-to-balloon” times minimizes tissue death and drastically improves survival odds.

The four links of the American Heart Association STEMI Chain of Survival.
The American Heart Association STEMI Chain of Survival illustrates responder actions when a patient may be experiencing ACS2. The links are:
- Rapid recognition and reaction to STEMI warning signs.
- Rapid EMS dispatch, EMS transport, and pre arrival notification to the receiving hospital.
- Rapid assessment and diagnosis in the ED or cath lab.3
- Rapid treatment which keeps in mind the role of family members and healthcare providers.
The FIRST link represents the interaction between the ACS symptomatic patient and the emergency dispatcher. Depending on local jurisdiction protocols, trained dispatchers may recommend over-the-counter emergency medications over the phone.
For example, dispatchers can recommend aspirin to ACS patients, but they should be able to assess the patient accurately through the phone and make sure that the patient has no obvious contraindications to taking aspirin (such as severe allergies or active gastrointestinal bleeding).
What treatments are included in the ACS algorithm?
Regardless of whether the patient is ultimately diagnosed with a STEMI or a lower-risk event, the immediate early intervention bundle remains consistent for suspected ACS. Providers should administer therapies based on the following general guidelines (always adhering to their local protocols):
- 12-Lead ECG: Acquire within 10 minutes to rapidly identify STEMI.
- Oxygen: Administer supplemental oxygen only if the patient’s O2 saturation is below 90%, they are in respiratory distress, or exhibit signs of heart failure.
- Aspirin: Administer 162 to 325 mg of chewable, non-enteric-coated aspirin to prevent further platelet aggregation and clot expansion.
- Nitroglycerin: Give sublingual nitroglycerin (0.4 mg) every 5 minutes up to 3 doses to reduce preload and relieve ischemic pain, provided the patient is not hypotensive or recently used phosphodiesterase inhibitors (e.g., Viagra).
- Morphine: Consider IV morphine strictly as a secondary measure if chest pain is unrelieved by nitroglycerin, noting that recent evidence suggests it may delay the absorption of other critical antiplatelet medications.
Summary
Chest pain, pressure, and tightness are hallmark symptoms of ACS. Patients may feel ischemic pain radiating throughout their jaw, arms, shoulders, and back. Responders must know how to recognize these symptoms rapidly to trigger the ACLS chest pain algorithm and engage the STEMI Chain of Survival.
Once the pathway is triggered and early interventions (Oxygen, Aspirin, Nitroglycerin, Morphine) are considered, the pivotal decision point relies entirely on acquiring an early 12-lead ECG. The ECG dictates the workflow, immediately routing the patient into a STEMI, NSTE-ACS, or Low-Risk ACS treatment branch to ensure timely reperfusion therapy and prevent permanent cardiac damage.
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
1. Mayo Clinic. Acute Coronary Syndrome. 2021.
2. American Heart Association. Systems of Care for ST-Segment–Elevation Myocardial Infarction: A Policy Statement From the American Heart Association. 2021.
3. Journal of the American Heart Association. Performance of Emergency Department Screening Criteria for an Early ECG to Identify ST‐Segment Elevation Myocardial Infarction. 2017.
More to Learn
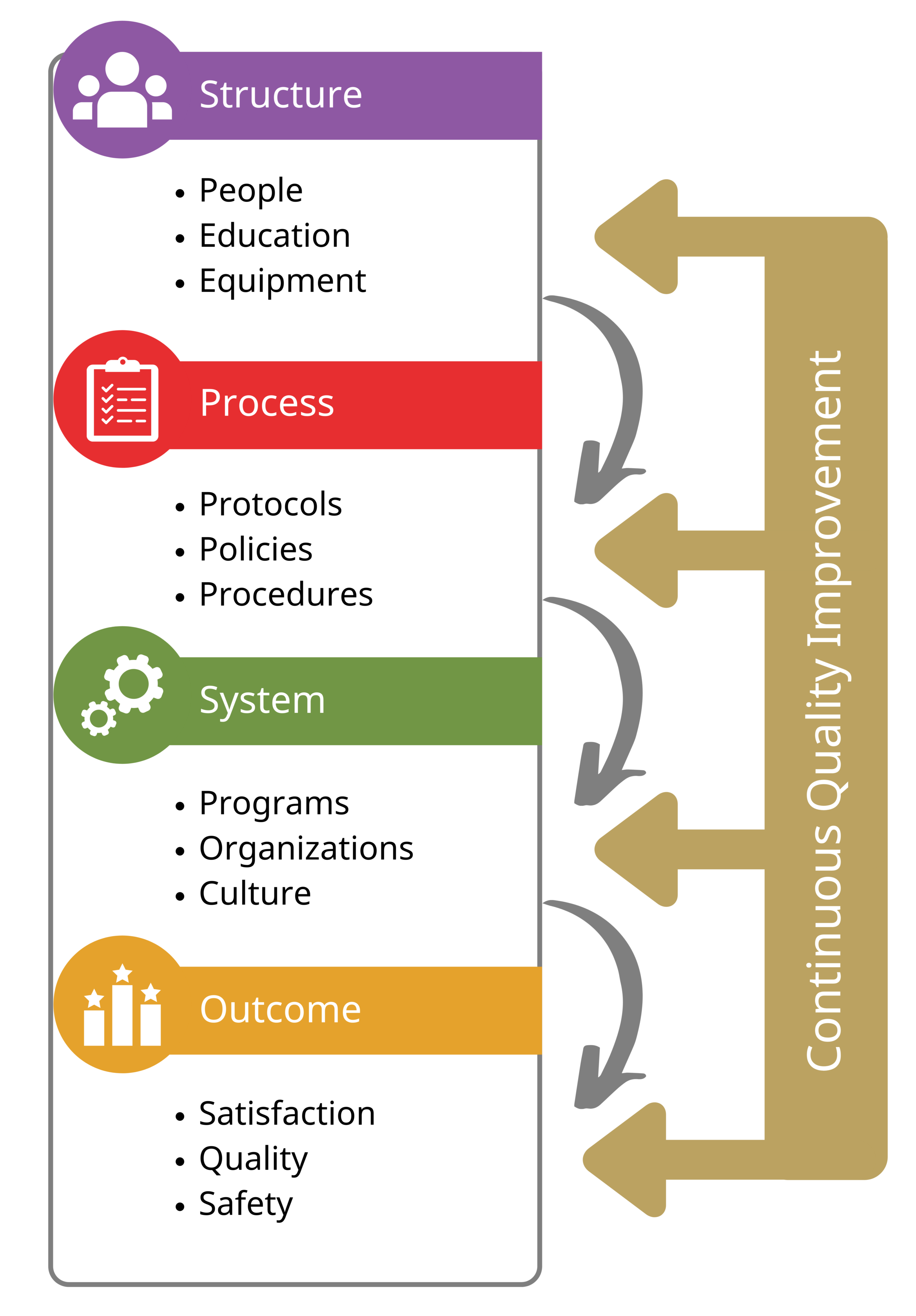
In-Hospital Cardiac Arrest Care is the first aspect of the system of care, a framework for linking the interdependent components of healthcare institutions' resuscitation system.
Keep your life-saving skills current with the 2019 AHA focused update on advanced cardiovascular life support. Learn how to use advanced airways, vasopressors, and extracorporeal cardiopulmonary resuscitation during cardiac arrest.