Systems of Care: In-Hospital Cardiac Arrest
This guide explores the interdependent components of an In-Hospital Cardiac Arrest (IHCA) system of care. Designed for hospital administrators, ACLS providers, and rapid response teams, this article will teach you how to evaluate your current protocols, identify weak points in your chain of survival, and implement continuous quality improvements to optimize patient outcomes.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Table of Contents
- IHCA System of Care: Why It Matters and Where Breakdowns Happen
- Pre-Arrest Rapid Response Systems
- Continuous Quality Improvement (CQI)
- Activating the IHCA SOC
- Crisis Resource Management
- The Resuscitation Team
- Acute Life-Threatening Events Recognition and Treatment (ALERT) Program
- Debriefing
- Post-Cardiac Arrest Care
- Summary
Article at a Glance
- The Framework: Systems of care link structure, process, and system components to achieve optimal survival rates.
- IHCA vs. OHCA: In-hospital and out-of-hospital cardiac arrests have distinctly different chains of survival and resource availabilities.
- Pre-arrest Response: Early recognition via scoring tools (like NEWS) and rapid response team activation are critical to preventing IHCA.
- Continuous Quality Improvement (CQI): Utilizing models like Plan-Do-Check-Act alongside hot and cold debriefings drives better future performance.
- Post-cardiac arrest syndrome is treated in the post-cardiac arrest phase, increasing the likelihood of survival and discharge with optimal neurologic function.
Systems of care (SOC) is a framework for linking the interdependent components of the resuscitation system of healthcare institutions.1 It identifies the strengths and weaknesses of current protocol to make improvements. SOC should increase the probability of successful resuscitation.

Systems of Care Taxonomy
What Are the Elements of a System of Care ACLS?
To be effective, an ACLS system of care must integrate four key elements:
Structure
This is the foundation. It includes competent personnel, proper resuscitation equipment, and necessary ongoing training and education.
Process
This involves how the structure is used. Processes are the protocols, organizational programs, and cultures established to deliver the highest quality of healthcare.
System
The system is the interdependent sum of the structure and process. It must be continuously evaluated and improved based on gathered data, experiences, advances in technology, and the latest resuscitation research.
Patient Outcomes
The ultimate goal of the structure, process, and system is to achieve optimal patient outcomes, specifically increasing survival rates with favorable neurological function.
A system of care must have structure, including competent personnel, proper equipment, and necessary training and education, to create processes. The structure involves producing programs, organizations, and cultures to achieve optimal patient outcomes, strengthening the quality of healthcare delivery systems.
The structure, processes, and systems are continuously improved based on data gathered from the institution’s outcomes, experiences, advances in technology, and latest resuscitation research.
In-hospital cardiac arrest (IHCA) and out-of-hospital cardiac arrest (OHCA) are two major aspects of a SOC. They revolve around the adult chain of survival.2 How the IHCA System of Care Works (End-to-End Flow):
- Surveillance: Staff monitor patients using early warning signs to detect deterioration.
- Activation: The Rapid Response Team (RRT) is called to intervene before arrest occurs.
- Resuscitation: If arrest occurs, the code team delivers high-quality CPR, rapid defibrillation, and ACLS.
- Post-Arrest Care: The patient is transferred to the ICU for targeted temperature management and hemodynamic optimization.
- Debriefing & CQI: The team reviews the event data to improve future performance.
American Heart Association (AHA) guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiovascular Care (ECC) provide system-specific chains of survival for IHCA and OHCA.

IHCA Chains of Survival

OHCA Chains of Survival
IHCA patients require instant access to additional trained hospital personnel. The first link in the IHCA chain of survival is a magnifying glass, representing the availability of effective surveillance and cardiac monitoring systems to avoid IHCA.
The telephone represents the cardiac arrest emergency response team, involving trained advanced cardiac life support (ACLS) providers such as doctors, nurses, respiratory therapists, and others. Hospitals must implement accessible and efficient methods of activating the emergency response team.
After notifying the team, clinicians administer high-quality CPR, rapid defibrillation, and ACLS support with post-cardiac arrest care, represented via the hand, heart, and hospital bed. Readers who need a clearer comparison of these first two actions can review defibrillation vs CPR. The final step in the IHCA is a multidisciplinary plan for recovery and rehabilitation after discharge from the inpatient hospital stay.
OHCA is more challenging due to the lack of trained personnel and limited space for ACLS equipment. OHCA depends on community training instead of healthcare workers. A trained lay rescuer must recognize and perform the appropriate steps when there is a cardiac arrest outside the hospital setting, represented by the telephone and hands.
Rapid defibrillation is also recommended if an automated external defibrillator (AED) is available, represented by a heart on the chains of survival. When emergency medical services arrive, they take over the rescue sequence, as seen by the ambulance.
EMS delivers the patient to the appropriate healthcare institution, so they can undergo further treatment such as cardiac catheterization or ICU admission. That is represented by the hospital bed. The final step in the OHCA is a multidisciplinary plan for recovery and rehabilitation after discharge from the inpatient hospital stay.
Ideally, all bystanders will know how to perform high-quality CPR and immediate defibrillation, increasing the patient’s chances of survival.

The community, EMS, and hospital systems are interlinked. The hospital is the final destination.
IHCA System of Care: Why It Matters and Where Breakdowns Happen
Respiratory failure and circulatory shock cause most IHCA incidences, with circulatory collapse often linked to different types of shock. Prompt treatment requires early recognition of respiratory distress, signs of shock, and neurologic deterioration. Clinicians typically admit IHCA patients to a highly monitored intensive care setting.
According to the AHA’s “Get With The Guidelines” program, structured systems of care have driven a measurable 4–8% increase in survival to hospital discharge rates amongst in-hospital CPR patients.
Improvement strategies also play an important role in preventing cardiac arrest and increasing survival rates. According to AHA data, 19% of in-hospital CPR occurred in unmonitored general wards, compared to 48% in the intensive care units (ICU) and 18% in the emergency departments (ED). Most hospitals provide teams and optimized SOC for patients in the ICU and ED.3
There are still gaps in healthcare SOC. Studies show a decrease in resuscitation outcomes during the nighttime, weekends, and holidays. Lower-income patients also have lower survival rates after IHCA.
Read: General Stroke Care
Pre-Arrest Rapid Response Systems
The goal of a pre-arrest rapid response system is to intervene before cardiopulmonary resuscitation is necessary. A standard pre-arrest escalation checklist connects early recognition to immediate action:
- Recognize: The bedside nurse or clinician notes abnormal or critical vital signs.
- Score: The clinician calculates the score using tools like the National Early Warning Score (NEWS) or a hospital-specific Early Warning Sign System (EWSS).
- Activate: If the score breaches the established threshold, the rapid response team (RRT) or medical emergency team (MET) is activated.
- Intervene: The RRT/MET assesses and stabilizes the patient, potentially transferring them to the ICU.
1. Recognition of Patients at Risk for Cardiac Arrest
Hypovolemic shock and respiratory failure are the most common IHCA causes. These patients present with tachypnea, tachycardia, and hypotension.
Cardiac arrest commonly occurs in non-specialized hospital wards, such as general surgical or medical wards. It’s likely due to the lack of monitoring equipment and specialized personnel. Studies show personnel in the medical and surgical wards don’t report abnormal or critical vital signs in 10% of patients.
Common Monitoring Misses in General Wards:
- Infrequent vital sign checks resulting in missed abnormal vitals.
- Delayed escalation due to alarm fatigue or unclear thresholds.
- Failure to recognize slow, progressive trends in deterioration.
Critical care areas have a higher nurse-to-patient ratio and specialized monitoring equipment. Frequent monitoring is possible and clinicians quickly recognize the first signs of instability. Monitoring strategies must be advanced via more accessible advanced monitoring equipment. Quick assessment tools may also be utilized to clinically monitor patients for early warning signs of cardiac arrest, such as the National Early Warning Score (NEWS) and Early Warning Sign System (EWSS).
2. Rapid Response Teams, Medical Emergency Teams, and Early Warning Sign Systems
The rapid response team (RRT) and the medical emergency team (MET) intervene in IHCA patient care. They’re composed of physicians, nurses, and respiratory therapists. They’re available around the clock and are equipped with advanced tools for monitoring and resuscitation. RRTs and METs reduce cardiac arrest incidence, especially in general wards.
Early Warning Sign Systems (EWSS) are scorecards grading the severity of a patient’s critical condition, reducing incidences of cardiac arrest. They require mandatory actions based on the scoring and are displayed for easy nurse access.
Examples of RRT/MET Activation Criteria & Response Actions:
- Criterion: Sustained tachycardia > 130 bpm or severe bradycardia < 40 bpm. Action: Assess rhythm, administer appropriate rate-controlling or chronotropic medications, and attach continuous monitoring.
- Criterion: Acute drop in oxygen saturation (SpO2 < 90%) despite oxygen therapy. Action: Evaluate airway, initiate advanced non-invasive ventilation (e.g., BiPAP), and prepare for intubation if necessary.
- Criterion: Sudden, acute change in mental status. Action: Assess neurologic baseline, check blood glucose, and prepare for emergency imaging (CT scan).
3. Continuous Assessment
When a critical patient is treated, the RRTs and METs perform continuous assessment until the patient is stabilized. If the patient is not improving or has a high risk of IHCA, they are transferred to the ICU for close monitoring.
Studies show if critically ill patients are not promptly transferred to the ICU, they have a high chance of mortality. Continuous assessment prevents further deterioration to cardiac arrest.4
4. Do not Resuscitate and Palliative Care
Some situations require clinicians to allow the natural process of death, such as when a medically insurmountable condition prevents life or a good quality of living. In such cases, RRTs focus on palliative care after obtaining advanced directives and do not resuscitate orders.
Clinicians must seek family input regarding aggressive resuscitation measures if it wasn’t discussed before the event.
Continuous Quality Improvement (CQI)
To continually improve, resuscitation teams must evaluate their systems through measuring key performance indicators (KPIs), comparing and analyzing data, and creating new interventions to improve outcomes. Relevant IHCA SOC KPIs include RRT activation timing, time to first defibrillation, CPR quality metrics (such as compression fraction), and debrief completion rates.
A primary method for organizing this feedback loop is the “PLAN-DO-CHECK-ACT” (PDCA) model. Through PDCA, feedback directly alters training strategies, optimizes equipment placement, and refines processes to ensure teams maintain well-choreographed ACLS, high-quality CPR, and early defibrillation for optimal outcomes.

Plan-Do-Check-Act
Activating the IHCA SOC
While the most common way to call the RRT or MET teams is via the hospital’s public address system, modern frameworks use multiple pathways. Common activation methods include:
- Dedicated “Code Blue” or emergency buttons located in patient rooms.
- Direct dial emergency extension numbers routing straight to the switchboard.
- Automated mobile alerts sent directly to RRT members’ devices based on EWSS scoring.
Additionally, hospitals must implement strict policies defining speed expectations and target response times, ensuring the team arrives at the bedside as rapidly as possible to improve the team’s overall timing.
Crisis Resource Management
Resuscitation teams perform their best when applying CRM principles. Each member must:
- Identify the single team leader explicitly.
- Know and stay within their assigned role boundaries.
- Execute seamless, coordinated teamwork.
- Use closed-loop communication (e.g., repeating a medication order back to the leader before and after administration).
To support role clarity and CRM principles, clinicians and institutions must:
- Emphasize and require specific training for the ACLS team leader role.
- Implement cognitive checklists for leadership activities (like the H’s and T’s).
- Standardize communication protocols between team members.
- Perform rigorous cross-checks to ensure the safety of team members before defibrillation.
The Resuscitation Team
Resuscitation team personnel must maintain adequate training and retraining skills to minimize errors and optimize patient outcomes. The core resuscitation team (often referred to as the code team) is typically composed of physicians, nurses, and trained ancillary healthcare workers such as respiratory therapists and pharmacists. Some institutions also utilize other personnel, such as security guards, clergy members, and social workers.
To minimize errors during chaotic emergencies, highly effective teams designate clear responsibilities:
- Team Leader: Directs the code and makes all critical medical decisions.
- Compressor: Performs high-quality chest compressions.
- Airway: Manages the BVM and advanced airway placement.
- Defib/Monitor: Operates the manual defibrillator or AED.
- Medications: Obtains IV/IO access and pushes required drugs.
- Recorder: Tracks times, shocks, rhythms, and medications.
As part of the SOC structure, many hospitals use standardized role cards and physical floor-placement guidance to ensure everyone knows where to stand. Each team member frequently practices resuscitation procedures, including just-in-time or just-in-place training on a mannequin. Other training involves an interdisciplinary ACLS approach utilizing face-to-face lectures and hands-on simulations, supervised by an expert physician.
The ALERT program teaches early identification and rapid intervention for pre-arrest patients. It trains personnel to prevent further deterioration of critically ill patients, even if early interventions were already performed. Studies show this course of action reduces the number of patients with IHCA and improves rates of survival to hospital discharge. The system is continuous and interval training updates are required. This training requires face-to-face lectures and simulations. It is designed around individual wards of the hospital, increasing familiarization and improving team effectiveness whenever they respond to cardiac arrest. The course encourages participants to be proactive in identifying where they can reflect and improve on their actions.Acute Life-Threatening Events Recognition and Treatment (ALERT) Program
Debriefing
Debriefing encourages continuous improvement of the resuscitation team. Crucially, the outcomes of these debriefs directly feed into CQI metrics and the Check and Act phases of the PDCA cycle.
The hot debriefing is conducted right after a resuscitation effort, so team members’ memories are still fresh. A simple, reusable hot debrief template includes:
- What went well during the resuscitation?
- What needs immediate improvement?
- Were there any equipment or medication delays?
Some challenges may occur during hot debriefs, such as when physicians and nurses are unavailable because they’re administering post-cardiac-arrest care. Team members may also have a difficult time narrating information regarding the events that took place, particularly if the resuscitation did not end well.
The cold debriefing is performed later (several hours to a few days), allowing team members time to reflect and prepare. Plus, all team members can be present for the activity. Other experts may be invited to conduct a multidisciplinary assessment of the situation. A cold debrief takes a deeper dive into the monitor data (e.g., CPR fraction, time to shock) to discover systemic issues requiring broad protocol updates.
Post-Cardiac Arrest Care
When the patient achieves a return of spontaneous circulation (ROSC) after cardiac arrest, clinicians start post-cardiac arrest care. Cardiac arrest patients usually present with complications affecting the normal pathophysiologic process, known as post-cardiac arrest syndrome (a complex combination of brain injury, myocardial dysfunction, and systemic ischemia/reperfusion response), which is a major factor in patient mortality. While achieving ROSC is a victory, only 32% to 54% of these IHCA patients achieve survival to hospital discharge.6
Post-cardiac arrest care optimizes the patient’s hemodynamics (blood pressure and perfusion), treats precipitating factors (like a blocked coronary artery), and implements targeted temperature management (cooling the patient to protect brain function) with the goal of addressing the effects of post-cardiac arrest syndrome.
It’s recommended that clinicians refer these patients to a multidisciplinary team of specialists. If a hospital is not equipped to provide these services (e.g., lacking a cath lab or specialized ICU), its SOC should address the seamless transfer to more specialized institutions. A transfer-readiness checklist ensures transport teams are mobilized early, transport agreements are pre-established, and critical patient records are sent without delay.

Complications after a cardiac arrest are known as post-cardiac arrest syndrome.
Summary
Modern resuscitation relies on distinct, optimized systems care frameworks for IHCA and OHCA. While OHCA relies heavily on bystanders to recognize the emergency, call 911, and perform high-quality CPR before EMS arrival, an effective IHCA system focuses on preventing the arrest entirely.
By establishing strong structures (personnel and equipment) and processes (EWSS scoring, rapid response teams, and CRM), hospitals can drastically improve patient outcomes. Following an event, implementing rigorous hot and cold debriefings drives the continuous quality improvement (PDCA) cycle required to elevate survival rates.
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
1. American Heart Association. Systems of Care. 2020.
2. American Heart Association. Highlights of the 2020 AHA Guidelines Update for CPR and ECC. 2020.
3. Steven L. Kronick, Michael C. Kurz, Steve Lin, Dana P. Edelson, Robert A. Berg, John E. Billi, Jose G. Cabanas, David C. Cone, Deborah B. Diercks, James (Jim) Foster. Systems of Care and Continuous Quality Improvement. American Heart Association. 2015.
4. Matthew M Churpek, MD, MPH, PhD, Blair Wendlandt, MD, Frank J Zadravecz, MPH, Richa Adhikari, MPH, Christopher Winslow, MD, and Dana P Edelson, MD, MS. Association Between ICU Transfer Delay and Hospital Mortality: A Multicenter Investigation. National Library of Medicine. 2017.
5. Ulmer C, Miller Wolman D. System Strategies to Improve Patient Safety and Error Prevention. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. 2009.
6. Kelly N. Sawyer, Teresa R. Camp-Rogers, Pavitra Kotini-Shah, Marina Del Rios, Michelle R. Gossip, Vivek K. Moitra, Kirstie L. Haywood, Cynthia M. Dougherty, Steven A. Lubitz. Sudden Cardiac Arrest Survivorship: A Scientific Statement From the American Heart Association. American Heart Association. 2020.
More to Learn
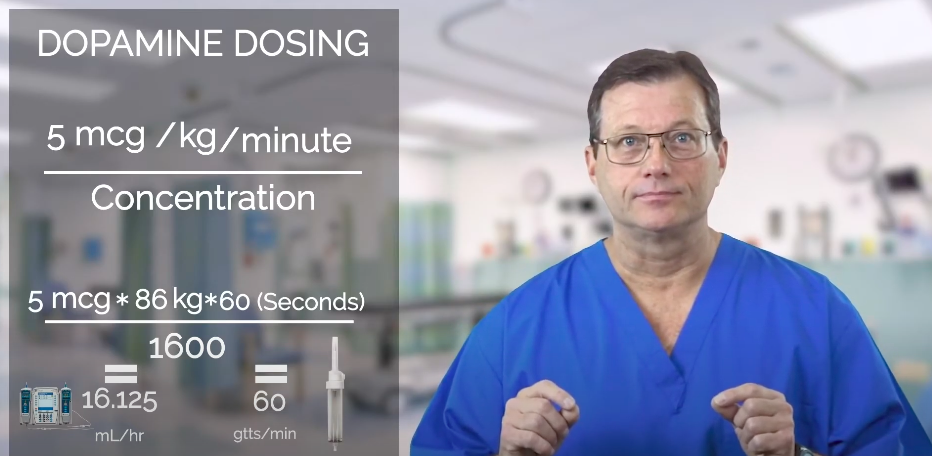
Learn how to accurately calculate dopamine infusions using the dopamine calculation. Our article helps you understand the dosing and administration guidelines for this medication.
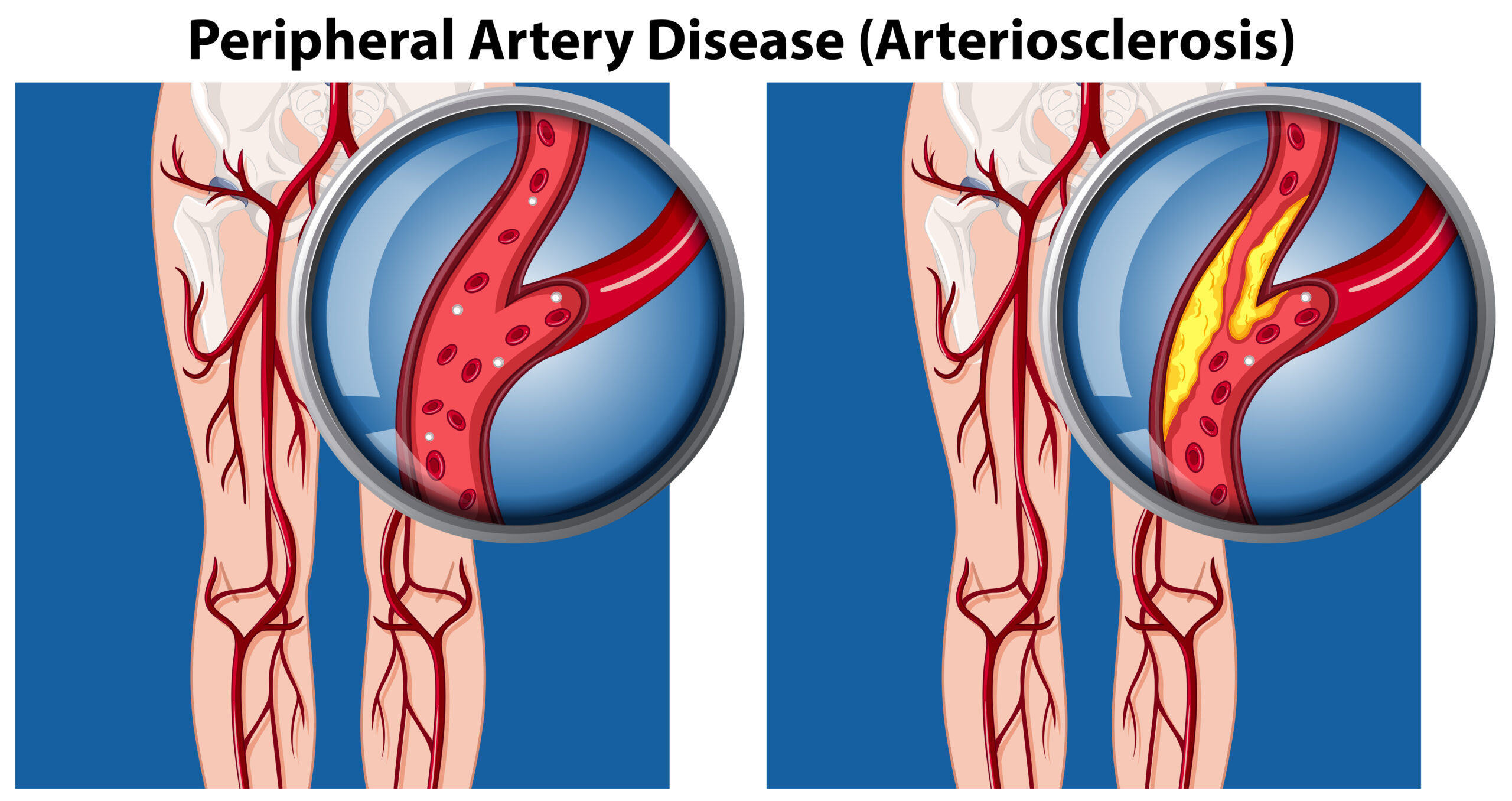
Explore Peripheral Vascular Disease in this detailed article and video. Learn about the pathophysiology of PVD and peripheral...