Acute Coronary Syndrome – The ACS Algorithm
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- The Acute Coronary Syndromes include STEMI, NSTEMI, and unstable angina.
- A 12-lead ECG helps distinguish among the ACS categories.
- Pre-hospital acute coronary syndrome treatment is essential to reducing morbidity and mortality.
- Timely reperfusion therapy increases survival rates.
Introduction
Clinicians must know how to identify and manage patients with acute coronary syndromes (ACS). Patients with acute myocardial ischemia (unstable angina), non-ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI) fall under the ACS umbrella.
Common Symptoms of Acute Coronary Syndrome
Patients with ACS can present with classic symptoms or more subtle complaints. In addition to general chest discomfort, clinicians should actively screen for associated symptoms and “anginal equivalents,” especially in older adults, women, and patients with diabetes.
- Chest discomfort: pressure, tightness, squeezing, heaviness, or burning (may come and go)
- Radiation: pain to the left/right arm, shoulder, neck, jaw, or back
- Shortness of breath (with or without chest discomfort)
- Diaphoresis (sweating), nausea/vomiting, lightheadedness, or syncope
- Fatigue/weakness or atypical epigastric discomfort (“indigestion”)

Acute coronary syndromes include STEMI, NSTEMI, and unstable angina, heart conditions associated with sudden, reduced blood flow to the heart.
A 12-lead ECG helps clinicians distinguish one condition from another. Based on ECG results, a patient with ACS may be diagnosed with: (1) ST-segment elevation with ongoing acute myocardial infarction, (2) ST-depression myocardial ischemia, or (3) non-diagnostic or normal ECG.
Early ACS management via reperfusion intervention is critical to treatment success. Acute ischemia may rapidly progress, resulting in sudden cardiac arrest or hypotensive bradyarrhythmia.1 In these emergencies, providers should quickly transition to the ACLS cardiac arrest circular algorithm to guide high-quality CPR, defibrillation, and medication management. Providers must be prepared with appropriate bradyarrhythmia treatment strategies in these cases.
Clinicians must examine the patient’s clinical history, physical examination, and 12-lead ECG findings to anticipate treatment strategies. Treatment may involve defibrillation, drug therapies, and pacing for symptomatic bradycardia.

A 12-lead ECG helps clinicians determine the type of acute coronary syndrome.
Read: Cardiac Arrest Circular Algorithm Explained
The Acute Coronary Syndrome Algorithm
Assessing the Patient for Symptoms
Before moving through the algorithm steps, confirm the symptom profile and timing. Acute coronary syndromes algorithm pathways are driven by the patient’s clinical presentation and the earliest ECG findings, so a focused symptom assessment helps determine urgency and the next best intervention.
- Confirm onset time: when symptoms began and whether they are ongoing
- Characterize pain: pressure vs sharp pain, radiation, severity, and triggers
- Associated symptoms: dyspnea, diaphoresis, nausea, syncope, palpitations
- Risk factors/history: prior MI/PCI/CABG, diabetes, smoking, HTN, HLD, family history
- Immediate red flags: hypotension, altered mental status, pulmonary edema, shock
Tip: obtain a 12-lead ECG as early as possible and repeat it if symptoms persist and the first ECG is non-diagnostic.
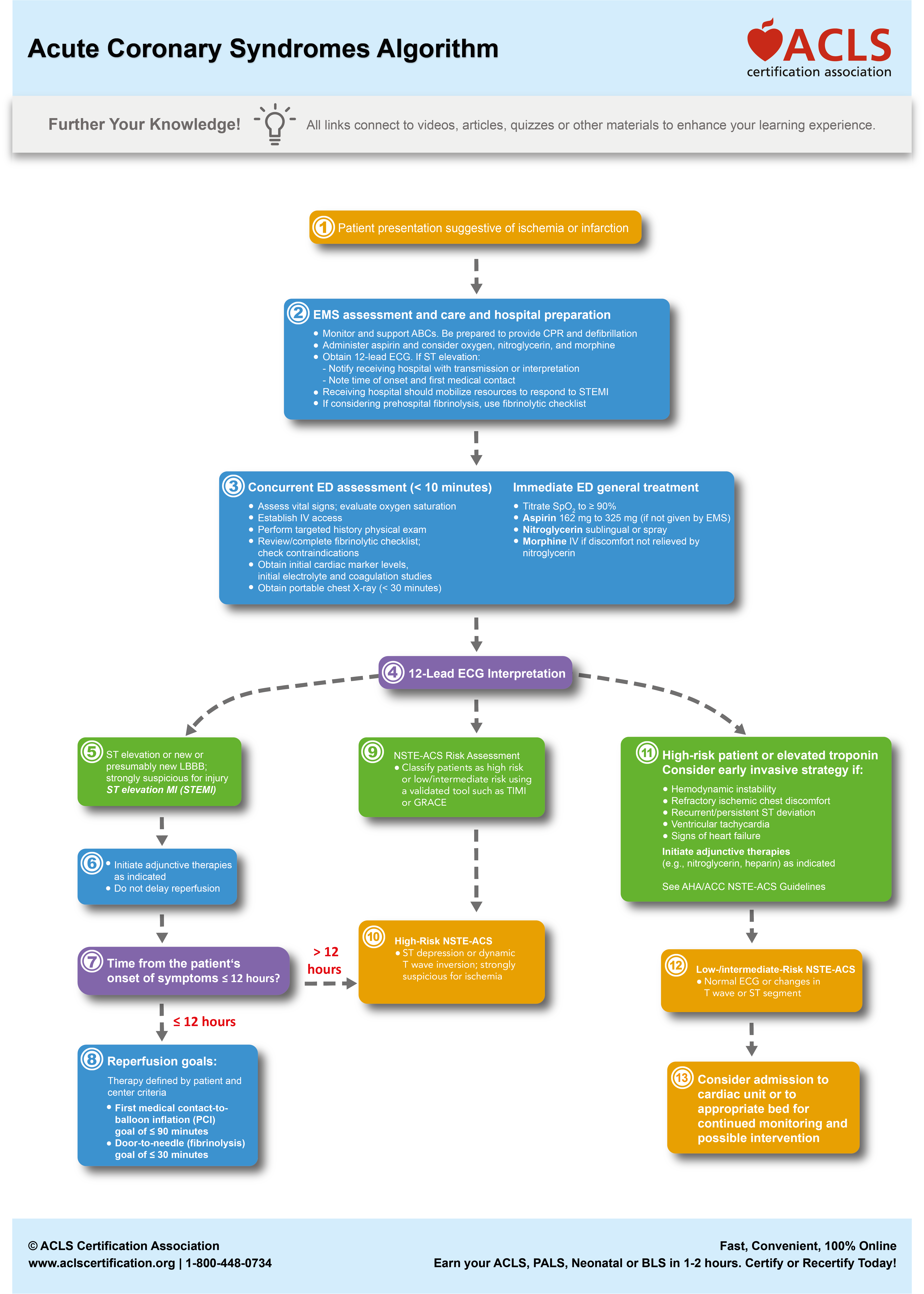
Clinicians should follow the Acute Coronary Syndrome Algorithm to direct treatment.
The Difference Between STEMI and NSTEMI in ACS
STEMI is typically caused by a complete coronary artery occlusion and is identified by ST-segment elevation (or a STEMI equivalent) on the ECG. Because myocardium is at immediate risk, the algorithm prioritizes rapid reperfusion (PCI preferred; fibrinolysis when PCI is not timely/available).
NSTEMI is usually due to partial occlusion or severe demand ischemia. ECG findings may include ST-segment depression, T-wave inversion, or a non-diagnostic tracing. Management focuses on anti-ischemic therapy, antiplatelet/anticoagulation strategies, risk stratification, and early cardiology evaluation, with cath/PCI based on risk and clinical stability.
- Why it matters in the algorithm: STEMI → reperfusion pathway immediately; NSTEMI/UA → serial ECGs/troponins + risk-based invasive strategy.
- Key point: A normal ECG does not exclude ACS; repeat ECGs, and evaluate troponins when suspicion remains high.
Related Video – Understanding the Acute Coronary Syndrome Algorithm
Goals for Management of ACS Patients
ACS patients are prone to developing ventricular fibrillation (VF) during the first four hours after the onset of chest pain.2 VF or pulseless ventricular fibrillation (pVT), especially in the out-of-hospital cardiac arrest patient, may be fatal.

Ventricular fibrillation features a rapid and erratic heart rhythm.
Laypersons in the pre-hospital setting should be trained in basic life support (BLS) and first aid. Further, EMS must determine if the patient is experiencing myocardial infarction or another type of chest pain. If necessary, EMS performs early defibrillation with an AED.
The provider’s primary goal is to provide reperfusion therapy as soon as possible to increase survival rates.3
Reperfusion therapies dilate the occluded coronary artery (or arteries). It involves percutaneous coronary intervention, or stenting, and uses fibrinolytics and drug therapies which dissolve occlusion and improve blood flow to the myocardium.

A stent is placed in a coronary artery to reperfuse the heart.
The ACS algorithm shows responders the necessary steps to assess and manage patients presenting with ACS symptoms. In the prehospital setting, EMS is responsible for the immediate assessment and initial intervention.
ACS treatments may involve the use of oxygen supplementation, aspirin, nitroglycerin, and morphine. Understanding the benefit of morphine for acute coronary syndrome helps providers optimize pain relief and reduce sympathetic drive during ischemia. EMS must quickly record the patient’s 12-lead ECG to inform hospital clinicians and other field EMS what intervention they should perform next.
Depending on the 12-lead ECG findings, responders may start adjunctive therapies or perform a reperfusion intervention, such as administration of a fibrinolytic. Some patients may require close monitoring and serial troponins to rule out ACS.
Responders have a checklist to evaluate if the patient can undergo medical treatment by fibrinolysis.
The ACS algorithm aims to triage patients based on symptoms and the ECG interpretation.4 Clinicians may request tests when the patient arrives at the hospital. For example, providers should order labs, which may include CK-MB, troponin, coagulation studies, and other tests.
For STEMI patients, providers may administer fibrinolytic therapy or perform diagnostic coronary angiography with possible angioplasty.
Essential Interventions for STEMI management
STEMI care is time-sensitive. The priority is to recognize STEMI early and activate the reperfusion pathway while supporting oxygenation, circulation, and symptom control.
- Immediate actions: continuous monitoring, IV access, obtain/repeat 12-lead ECG, activate cath lab or STEMI alert
- Reperfusion: PCI as soon as possible when available; consider fibrinolysis when PCI is not feasible within an appropriate timeframe
- Anti-ischemic/support: aspirin, nitrates when appropriate, treat pain/anxiety, manage blood pressure and any signs of heart failure if present
- Manage complications: bradycardia, tachyarrhythmias, cardiogenic shock, acute heart failure
Antiplatelet and Anticoagulation Therapies Administered for ACS
Drug therapy for ACS typically includes antiplatelet agents and anticoagulation to reduce further thrombus formation, alongside therapies that relieve ischemia and stabilize the patient while definitive management is arranged.
- Antiplatelet: aspirin is foundational; many patients also receive a second antiplatelet agent (dual antiplatelet therapy) based on the ACS type and planned intervention
- Anticoagulation: commonly used in NSTEMI/UA and often in STEMI depending on the reperfusion plan and institutional protocol
- Adjuncts: nitrates for pain/ischemia (when appropriate), statin therapy, beta-blockers when indicated, and oxygen only when hypoxemic per current practice standards
Note: Medication choice and dosing vary by protocol, contraindications, and whether PCI or fibrinolysis is planned.
When should fibrinolysis protocols be initiated?
Fibrinolysis is considered for STEMI when a patient meets criteria and timely PCI is not available. The decision is driven by symptom onset time, ECG confirmation of STEMI, and a rapid screen for contraindications to thrombolytic therapy.
- Best candidates: confirmed STEMI with ongoing symptoms and no major contraindications
- Timing matters: earlier treatment is generally more effective; document symptom onset clearly
- Safety: use a structured contraindication checklist and monitor closely for bleeding complications
- Next step: after fibrinolysis, reassess ECG/symptoms and follow protocol for rescue PCI or transfer as indicated
Related Video – One Quick Question: What are ACLS Algorithms?
The three acute coronary syndromes are STEMI, NSTEMI, and unstable angina. It’s paramount that providers know how to read and interpret a 12-lead ECG to diagnose a patient, especially recognizing ST Segment Elevation as a hallmark of STEMI, while also monitoring for complications such as bradyarrhythmias. EMS and other providers must know how to treat an ACS patient in the prehospital setting. Keep in mind, reperfusion therapy increases survival rates.Summary
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
1. EuroIntervention. Cardiac arrhythmias in acute coronary syndrome. 2014.
2. Justine Bhar-Amato, William Davies, and Sharad Agarwal. Ventricular Arrhythmia after Acute Myocardial Infarction: ‘The Perfect Storm’. National Library of Medicine. 2017.
3. Eric R. Bates. Reperfusion Therapy Reduces the Risk of Myocardial Rupture Complicating ST‐Elevation Myocardial Infarction. Journal of the American Heart Association. 2014.
4. B. B. L. M. IJkema, J. J. R. M. Bonnier, D. Schoors, M. J. Schalij, and C. A. Swenne. Role of the ECG in initial acute coronary syndrome triage: primary PCI regardless of presence of ST elevation or of non-ST elevation. National Library of Medicine. 2014.
More to Learn
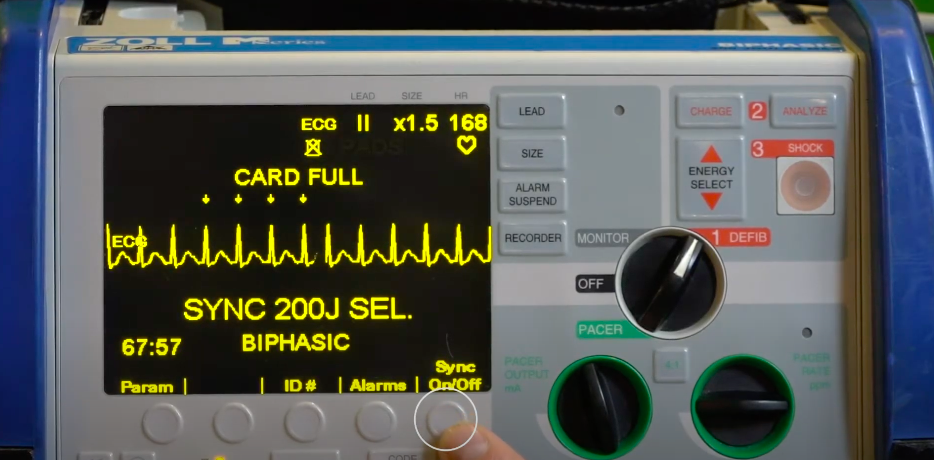
Learn the technique of synchronized cardioversion at ACLS Certification Association. Our article helps you acquire the skills to deliver effective electrical therapy.

Download the Cardiac Arrest Circular Algorithm PDF to learn the correct procedure to provide high-quality cardiopulmonary resuscitation using step-by step descriptions, Infographics, and Video Illustrations.