ACLS Cardiac Arrest Circular Algorithm Explained
This guide provides a comprehensive breakdown of the ACLS Cardiac Arrest Circular Algorithm. Designed for healthcare providers, EMS personnel, and ACLS learners, this article will teach you how to execute continuous 2-minute CPR loops, manage shockable versus nonshockable rhythms, and seamlessly integrate drug therapy and advanced airways without interrupting chest compressions.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- The 2-Minute Loop: The circular algorithm is built on uninterrupted, repeating 2-minute cycles of high-quality CPR interspersed with brief pulse and rhythm checks.
- Rhythm Decision Points: During the rhythm check, providers must explicitly identify if the rhythm is shockable (VF/pVT) or nonshockable (Asystole/PEA).
- Continuous Action: Chest compressions must resume immediately after a shock is delivered; do not pause to check for a pulse until the next 2-minute cycle is complete.
What is the Difference Between the Cardiac Arrest Algorithm and the Cardiac Arrest Circular Algorithm?
Both algorithms guide providers through the exact same life-saving ACLS protocols for managing a pulseless patient. The difference lies entirely in their visual presentation. The traditional Adult Cardiac Arrest Algorithm uses a vertical, branching flowchart that splits into shockable and nonshockable pathways. The Cardiac Arrest Circular Algorithm presents this same information as a continuous loop, emphasizing the non-stop, cyclical nature of 2-minute CPR intervals while drug administration and airway management happen simultaneously in the background.
Introduction to the Cardiac Arrest Circular Algorithm
The Cardiac Arrest Circular Algorithm guides providers on the correct procedures to provide high-quality cardiopulmonary resuscitation. Aligning with foundational basic life support, advanced cardiac life support, and published guidelines cardiopulmonary resuscitation protocols, it functions as a cardiopulmonary resuscitation emergency framework. It begins immediately after recognizing that a patient is in cardiac arrest (no pulse and no normal breathing). For a plain-language comparison of compressions and shocks, review the difference between CPR and defibrillation.

During cardiac emergencies, the Cardiac Arrest Circular Algorithm provides essential life-saving steps.
The Core Repeating Sequence:
- Initiate CPR: Begin chest compressions and ventilations immediately.
- Administer Oxygen & Attach Monitor: Apply oxygen delivery equipment and positive-pressure ventilation devices, such as an oxygen tank and a bag-mask device. Apply the manual or automated external defibrillator to the patient as soon as possible, minimizing interruptions in compressions.
- Interpret Rhythm: Perform a rhythm check immediately once connected. Identify if the rhythm is shockable (Ventricular Fibrillation [VF] or pulseless ventricular tachycardia [pVT]) or a nonshockable rhythm (Asystole or Pulseless Electrical Activity [PEA]).
- Act on Rhythm: Either shock the patient or resume CPR immediately, continuing the 2-minute cycle while managing drug therapy and advanced airways concurrently.
Defibrillation Workflow:
- If a shockable rhythm is present, charge the device.
- While charging, chest compressions and ventilations resume, following the adult cardiac arrest algorithm.
- As soon as the device is charged, clear the patient and administer the shock.
- Afterward, the provider immediately performs five cycles or two minutes of high-quality CPR. 1
| Rhythm Type | Rhythms Included | Immediate Action | Epinephrine Timing | Antiarrhythmic Use? |
|---|---|---|---|---|
| Shockable | VF, pVT | Defibrillate, then immediate CPR | After 2nd Shock | Yes (Amiodarone or Lidocaine after 3rd shock) |
| Nonshockable | Asystole, PEA | Immediate CPR (No shock) | ASAP | No |
Read: Acute Coronary Syndrome – The ACS Algorithm
Initiate CPR
To initiate CPR, the provider utilizes chest compressions. Using the two-handed technique, rescuers should remember to push hard and push fast in the center of the chest. Chest compressions are applied to the lower half of the sternum.
How is high-quality CPR performed in ACLS?
- Rate: Compress at a rate of 100–120 per minute.
- Depth: Depressions should be at least 2–2.4 inches (5-6 cm).
- Recoil: Allow for full chest recoil on the upstroke to permit heart filling.
- Minimize Interruptions: Keep pauses for ventilation or rhythm checks to an absolute minimum (under 10 seconds).
- Rotate Compressors: Rescuers must switch places to prevent rescuer fatigue. Once a rescuer feels arm strain and fatigue, the quality of chest compression decreases.

Chest compression technique is important. Push hard and allow the chest to recoil after each push.
Mastering the timing and depth of these compressions while coordinating with a partner is crucial. Review proper mechanics in our CPR for Adults with 2 Rescuers demonstration.
Administer Oxygen
When using a bag-mask device or other barrier device to provide positive-pressure ventilation, the rescuer should provide two breaths after sets of 30 chest compressions with 100% supplemental oxygen. This cycle is performed for 2 minutes. During this time, high-quality CPR should be maintained.2
Adjustments are made as needed. The provider should make sure compression depth, full chest recoil, and compression rate are being followed. When providing ventilations, the provider should ensure there is a visible chest rise as each breath is being provided. That is an indication that the ventilations are adequate.
Squeezing the bag too hard or too frequently can cause dangerous gastric inflation and decrease venous return to the heart. Deliver just enough volume to see chest rise, and ensure pauses for breaths remain extremely brief to minimize CPR interruptions.
To see how this is coordinated with compressions, watch our tutorial on Understanding Bag Valve Mask Usage During CPR.
Interpret Rhythm
After two minutes, the provider should perform a pulse and rhythm check. This pause must be less than 10 seconds.
When should defibrillation be used?
Defibrillation is exclusively used for shockable rhythms, specifically Ventricular Fibrillation (VF) or pulseless Ventricular Tachycardia (pVT), identified during a rhythm check. If the patient is in a nonshockable rhythm like Asystole or PEA, do not shock; instead, resume CPR immediately and focus on early epinephrine.
If there is no pulse but a shockable rhythm is present, ensure the patient is cleared and a shock is delivered. Chest compressions and ventilations are resumed immediately after giving the shock. Do not pause to check the pulse after shocking; wait until the end of the next 2-minute cycle.
Drug Therapy
Medication administration runs in the background of the circular algorithm without pausing CPR, a cornerstone principle of modern emergency cardiovascular care. The two primary medications used during cardiac arrest (and broader cardiovascular care scenarios) are Epinephrine (a vasopressor) and Amiodarone (an antiarrhythmic).
Intravenous Medications: Epinephrine
As the circular algorithm is repeated, the provider should consider gaining intravenous (IV) or intraosseous (IO) access for epinephrine. Once access is established, 1 mg of epinephrine is administered intravenously at a dilution of 1:10,000 followed by a bolus 10-mL normal saline flush. Because it is given every 3–5 minutes, many teams standardize this by administering Epinephrine every other 2-minute CPR cycle.
It is recommended to elevate the extremity where the IV access is in place while administering drugs in cardiac arrest patients. Also, drugs should be administered with chest compressions. These actions facilitate the flow of the drugs to the central circulation.
Intravenous Medications: Amiodarone
If the patient remains in a shockable rhythm after three shocks, amiodarone is initially administered at 300 mg intravenously followed by a 10-mL normal saline flush. (Note: Lidocaine at 1-1.5 mg/kg may be used as an alternative antiarrhythmic if Amiodarone is unavailable). Again, the extremity should be elevated and chest compressions continued when giving these drugs to facilitate transport to the central circulation. Subsequent doses of amiodarone can be given but at a lower dose of 150 mg.
Airway Management
Providers should consider inserting an advanced airway, such as endotracheal intubation with quantitative waveform capnography. Crucially, any advanced airway attempt must minimize interruptions in chest compressions.
Once the endotracheal tube is inserted, asynchronous ventilations can be performed. That means that while performing uninterrupted chest compressions, the rescuer should give one breath every six seconds timed at the full chest recoil of the chest compression phase.
Quantitative waveform capnography can be used to assess CPR quality. If the measured EtCO2 (PETCO2) concentration is below 10 mm Hg, then CPR techniques need improvement or there could be a problem with chest compressions and ventilation.
Cues for Return of Spontaneous Circulation (ROSC):
The favorable outcome in providing high-quality CPR is achieving a return spontaneous circulation (ROSC). Providers running the circular algorithm should watch for these signs, as achieving ROSC means the team will immediately transition into complex post-cardiac arrest care:
- Pulse: ROSC is confirmed if a palpable pulse and measurable blood pressure return.
- Capnography Spike: Quantitative waveform capnography will show a sudden, sustained increase of EtCO2 (PETCO2) concentration, often to more than 40 mm Hg.3
Reversible Causes of Cardiac Arrest
If a patient remains in cardiac arrest despite continuous cycles of CPR, defibrillation, and medication, the team leader must rapidly evaluate for underlying issues that can be fixed. These are known as the Hs and Ts:
The Hs:
- Hypovolemia: Severe fluid/blood loss; treated with IV fluids or blood.
- Hypoxia: Lack of oxygen; treated by securing the airway and ventilating.
- Hydrogen ion (acidosis): Severe acid buildup; treated with ventilation or sodium bicarbonate.
- Hypo-/Hyperkalemia: Potassium imbalance; treated with targeted electrolyte correction.
- Hypothermia: Severe core cooling; treated with active rewarming.
The Ts:
- Tension pneumothorax: Air trapped in the chest; treated with needle decompression.
- Tamponade (cardiac): Fluid crushing the heart, rapidly mimicking signs of right-sided heart failure and precipitating acute heart failure; treated with pericardiocentesis.
- Toxins: Drug overdose; treated with specific antidotes (e.g., naloxone).
- Thrombosis (pulmonary or coronary): Massive blood clots; treated with fibrinolytics or PCI.
Summary
The ACLS Cardiac Arrest Circular Algorithm provides a continuous, highly structured framework for managing pulseless patients. Once cardiac arrest is recognized, the team must immediately launch into uninterrupted 2-minute cycles of high-quality CPR. Providers pause only briefly at the end of each cycle to check the rhythm, deliver a shock if the rhythm is VF or pVT, and immediately resume compressions. In the background of this continuous loop, the team establishes IV/IO access, administers Epinephrine and Amiodarone at appropriate intervals, secures an advanced airway with waveform capnography, and actively diagnoses and treats any underlying Hs and Ts until ROSC is achieved.
More Free Resources to Keep You at Your Best
Editorial Sources
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
1. American Red Cross. AED Steps.
2. American Heart Association. ACLS Supplementary Material. 2012.
3. Bhavani Shankar Kodali and Richard D. Urman. Capnography during cardiopulmonary resuscitation: Current evidence and future directions. National Library of Medicine. 2014.
More to Learn
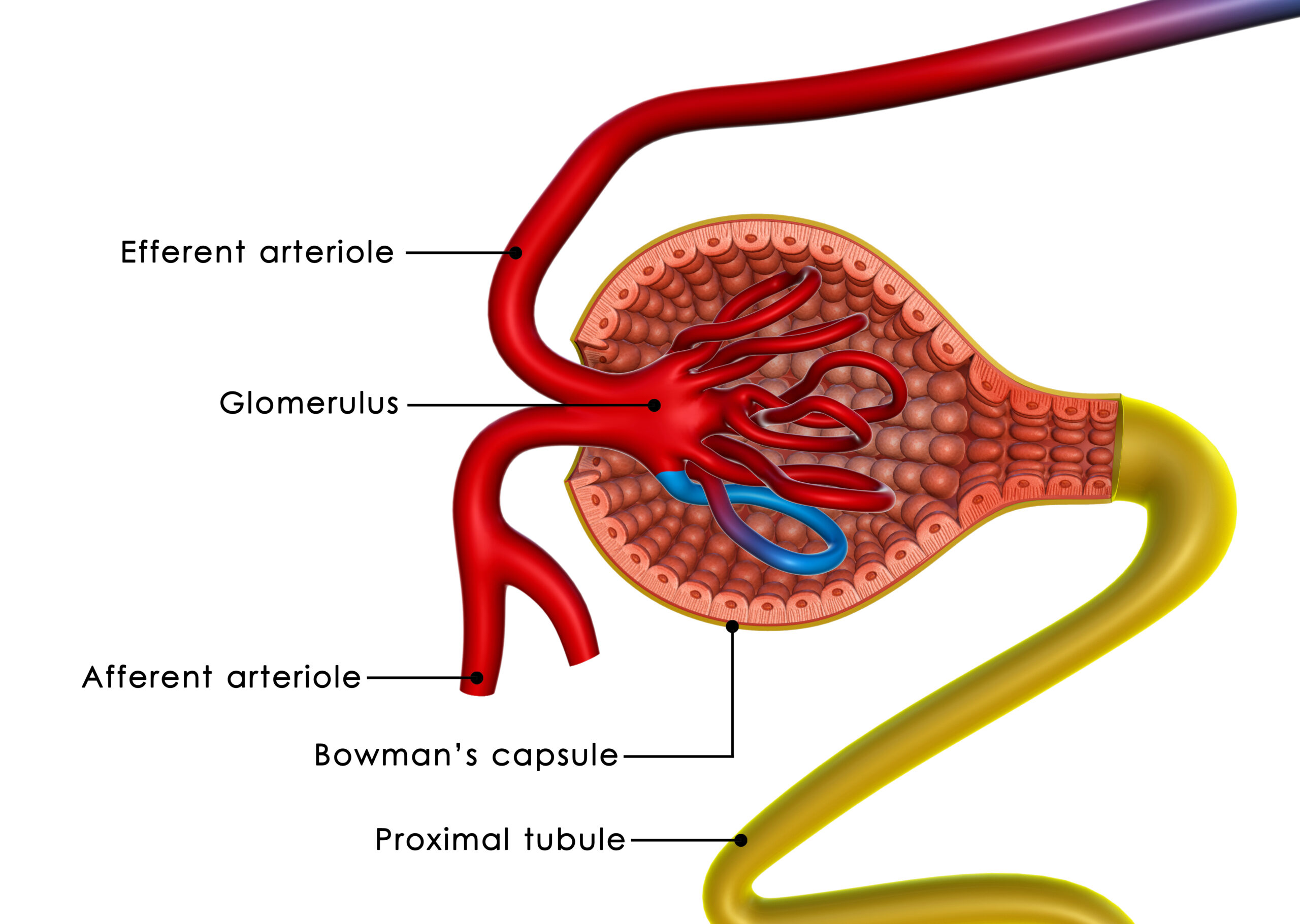
Read our detailed article and watch the video on Nephrotic Syndrome. Learn about nephrotic syndrome pathophysiology, signs, symptoms...
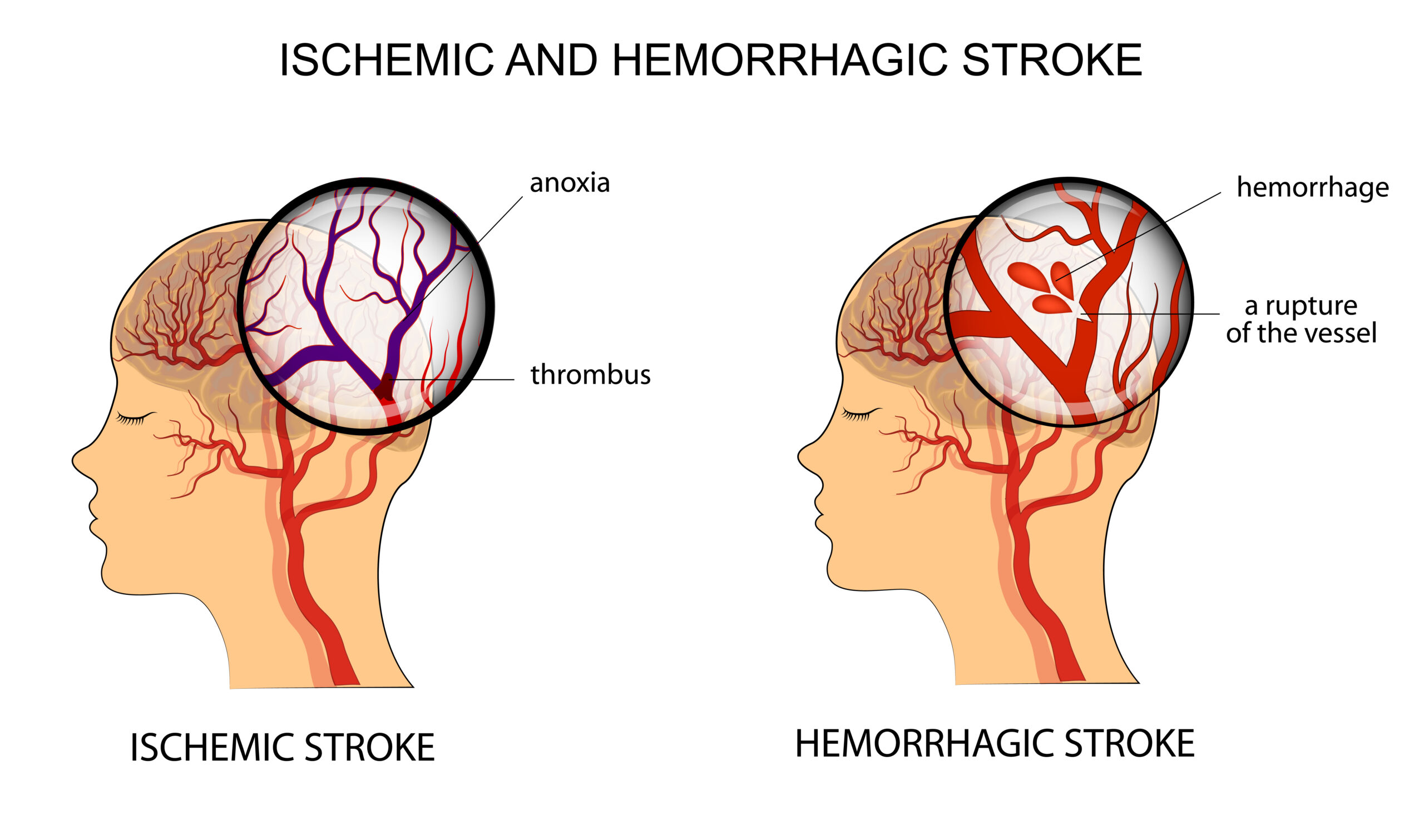
Learn the process of Acute Stroke Assessment in the Emergency Department. The general assessment is followed by Neurological assessment and determining ischemic or hemorrhagic stroke.