Overview of 2020 Changes
In 2020, the AHA and ILCOR released their full update for ACLS, BLS, PALS, and Neonatal Resuscitation. As has been true in the past, the group reviewed the strength of the recommendations and quality of supporting evidence to determine what interventions or strategies would be included. Unless changed or replaced in subsequent guidelines, these recommendations should be considered current.

The 2020 guidelines are a comprehensive revision of the AHA’s guidelines for adult, pediatric, neonatal, resuscitation education science, and systems of care topics.
Adult Basic and Advanced Life Support
The following section details the changes to ACLS protocols.
Changes in Visuals and Algorithms
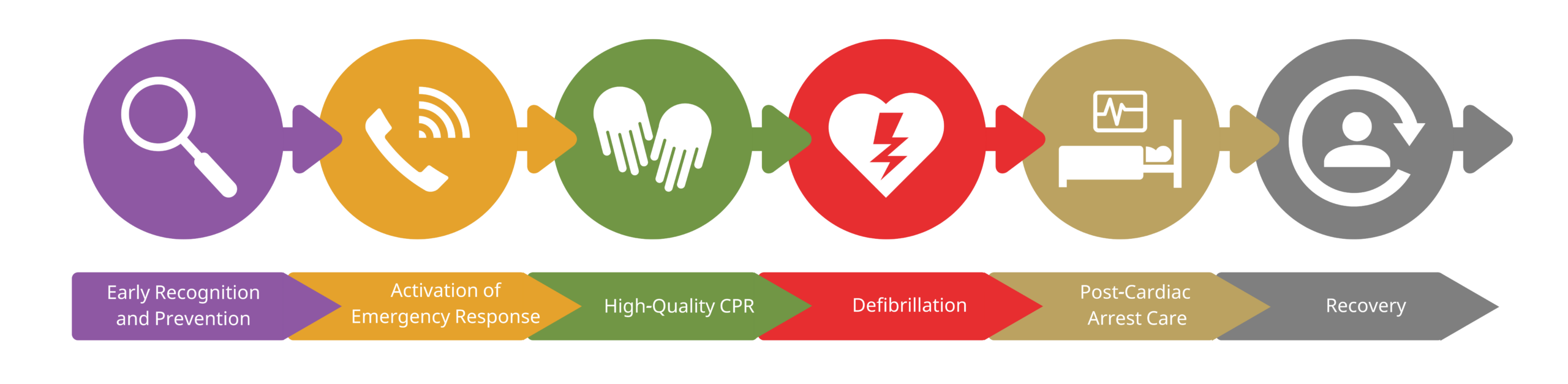
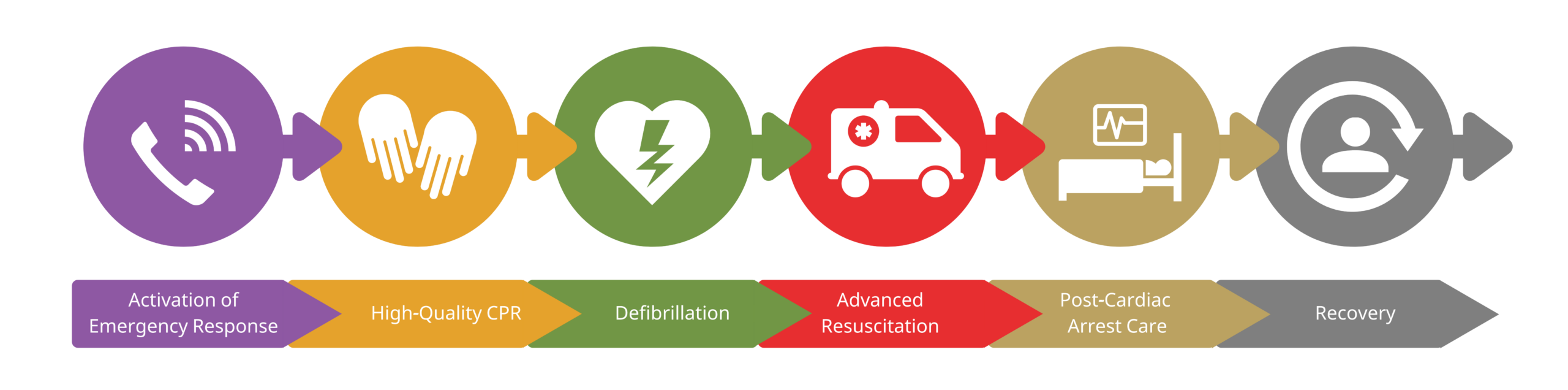
Addition of a recovery link in the IHCA and OHCA Chains of Survival.
- Modification to the Cardiac Arrest Algorithm to encourage early administration of epinephrine for nonshockable rhythms.
- New lay rescuer Opioid-Associated Arrest Algorithm.
- New trained rescuer Opioid-Associated Arrest Algorithm.
- Modification of the Post-Cardiac Arrest Care Algorithm to prevent hypoxemia, hypotension, and hyperoxia.
- New Cardiac Arrest in Pregnancy Algorithm.
- New visuals with information about neuroprognostication after the return of spontaneous circulation (ROSC).
Key Changes
In addition to the new algorithms and modifications to the existing algorithms, additional changes to the guidelines include:
- Lay rescuer initiation of cardiopulmonary resuscitation (CPR): AHA and ILCOR recommend that lay rescuers perform CPR on any person with presumed cardiac arrest.1 The risk of harm from CPR on a person not in a cardiac arrest is low.
- Early administration of epinephrine: For patients in nonshockable cardiac arrest rhythms, epinephrine should be administered as soon as possible. For those with a shockable rhythm, epinephrine may be administered if defibrillation is unsuccessful.
- Use of audiovisual feedback devices: The use of feedback devices may improve CPR performance and survival to hospital discharge.
- Monitoring of CPR quality: Improved data supports the use of arterial blood pressure and end-tidal CO2 monitoring (at least 10 mm Hg but > 20 mm Hg is ideal) to monitor the quality of CPR and improve the likelihood of ROSC.
AHA Chains of Survival. The 2020 guidelines add a recovery link in the In-Hospital Cardiac Arrest (IHCA) and Out-of-Hospital Cardiac Arrest (OHCA) Chains of Survival.
- Sequential defibrillation: There is no evidence to support applying two nearly simultaneous shocks for shockable rhythms in cardiac arrest.
- Intravenous (IV) access over intraosseous (IO) access: During cardiac arrest, IV access may be attempted first since the IV route has been found to have better clinical outcomes than the IO route. If an IV cannot be established, providers should consider IO access.2
- Support during recovery: This new guideline adds a recovery component to the IHCA and OHCA Chains of Survival. The recommendation includes rehabilitation assessment and treatment before hospital discharge for cardiac arrest survivors and their families. That includes cardiopulmonary, neurologic, return to work, post-traumatic stress, and assessment and treatment of fatigue.
- Lay rescuer debriefings: Although debriefings for providers have always been a recommendation, AHA and ILCOR now recommend debriefings for lay rescuers, emergency medical services (EMS) personnel, and hospital providers following a cardiac arrest.3
- Cardiac arrest during pregnancy: There is a new algorithm for the in-hospital pregnant patient in cardiac arrest. In the pregnant patient with cardiac arrest, airway and oxygenation management must be prioritized. Fetal monitoring should not be initiated. After ROSC, targeted temperature management should be initiated with continuous fetal monitoring for bradycardia.
Read: Understanding the 2019 AHA Updated Guidelines
Pediatric Basic and Advanced Life Support
The following are the AHA changes for PALS.
Changes in Visuals and Algorithms
- Addition of a Recovery link in the OHCA Chain of Survival.
- New Pediatric Chain of Survival for IHCA.
- Modification of the Pediatric Bradycardia with a Pulse Algorithm.
- Modification of the Pediatric Cardiac Arrest Algorithm to encourage early administration of epinephrine for nonshockable rhythms.
- Modification of the Pediatric Tachycardia with a Pulse Algorithm to include narrow and wide QRS complex tachycardias.
- New lay rescuer Opioid-Associated Arrest Algorithm.
- New trained rescuer Opioid-Associated Arrest Algorithm.
- New Pediatric Post-Cardiac Arrest Care Checklist.
AHA Chains of Survival for Pediatric In-Hospital Cardiac Arrest (IHCS) and Out-of-Hospital Cardiac Arrest (OHCA).
Key Changes
In addition to the new algorithms and modifications to the existing algorithms, additional changes to the pediatric guidelines include:
- Rescue breathing rate during assisted ventilation: For the pediatric patient with a pulse but inadequate respirations, AHA and ILCOR say it is reasonable to give one breath every 2–3 seconds instead of the old recommendation of one breath every 3–5 seconds.
- Ventilation during CPR with an advanced airway: During CPR with an advanced airway, the recommendation is to give one breath every 2–3 seconds (20–30 per minute) instead of the old recommendation of one breath every six seconds.
- Cuffed endotracheal tubes (ETTs): Cuffed ETTs should be used when intubating children and infants. The previous recommendation included the use of either cuffed or uncuffed tubes.
- Cricoid pressure: Routine cricoid pressure during intubation of children and infants is NOT recommended.4
- Early epinephrine administration: The AHA and ILCOR now recommend the early (within five minutes) use of epinephrine for nonshockable rhythms in cardiac arrest.
- Invasive blood pressure (BP) monitoring: When invasive blood pressure monitoring is in place in cardiac arrest, the provider can use the diastolic blood pressure to monitor CPR quality. The target for infants is 25 mm Hg and for children is at least 30 mm Hg.
- Seizures after ROSC: When available and in the presence of persistent encephalopathy, continuous electroencephalogram (EEG) monitoring should be in place to detect seizures after a pediatric cardiac arrest. Seizures and nonconvulsive status epilepticus should be treated in consultation with pediatric neurology experts.
- Support for cardiac arrest survivors: All pediatric cardiac arrest survivors should be assessed for the need for rehabilitation, including neurologic evaluation for at least one year after cardiac arrest.
- Fluid bolus in septic shock: Fluid overload during treatment for septic shock increases morbidity rates. Therefore, providers should use their best clinical judgment to determine if fluid boluses should be 10 mL/kg or 20 mL/kg.
- Vasopressors in septic shock: If fluid boluses are not successful in controlling pediatric blood pressure in septic shock, the provider can consider epinephrine or norepinephrine. In the absence of those medications, consider dopamine.
- Corticosteroids in septic shock: In the pediatric population, if the child in septic shock requires vasopressors, the provider should consider the administration of stress-dose corticosteroids.
- Hemorrhagic shock: For hemorrhagic shock following blood loss from trauma, the provider should consider administering blood products instead of crystalloid IV fluids.
- Opioid overdose: For pediatric patients with a suspected opioid overdose and resultant respiratory arrest, rescue breathing should be administered until spontaneous breathing begins. The child in respiratory arrest should receive intranasal or intramuscular naloxone. However, standard PALS measures (CPR) should be the priority for the child in suspected cardiac arrest.
- Myocarditis and cardiomyopathy: The acutely ill child with myocarditis should be transferred to ICU for treatment and monitoring. In the presence of low cardiac output, the provider should consider extracorporeal life support (ECLS). When cardiac arrest occurs in this population, consider extracorporeal CPR.
- Pulmonary hypertension: For the pediatric patient with pulmonary hypertension due to increased pulmonary vascular resistance (PVR), provide inhaled nitric oxide or prostacyclin. Avoid hypoxia and acidosis. Consider analgesics, sedation, or neuromuscular blocking agents for children at high risk for pulmonary hypertension.
Initial emergency treatment should include hyperventilation and increased oxygen to induce alkalosis while preparing for vasodilator administration. Consider ECLS for refractory pulmonary hypertension or low cardiac output despite treatment.
- Single Ventricle Stage 1 Norwood shunt: For children with this congenital heart disease, the AHA and ILCOR have added recommendations, including:
- Monitoring oxygen saturation by superior vena cava catheter
- Lowering systemic vascular resistance using vasodilators can increase oxygen delivery to the system in children with Norwood shunts
- In the presence of low delivery of oxygen following a stage 1 palliation, ECLS may be beneficial
- In suspected shunt obstruction, the clinician should order oxygen, vasoactive agents, and heparin in preparation for surgical intervention
- For neonates before surgical repair, target a PaCO2 of 50–60 mm Hg by reducing minute ventilation or providing sedation
- Single Ventricle Stages 2 and 3 Norwood shunt patients: For patients in later stages of management, recommendations include:
- For children in pre arrest and with severe hypoxemia, consider targeting a mild respiratory acidosis and a low mean airway pressure to increase oxygenation to the brain and other organs
- Consider ECLS as a temporizing measure until a ventricular assist device or surgical revision is available
Neonatal Life Support
The 2020 guidelines for neonatal support include recommendations for implementation of the Neonatal Resuscitation Algorithm, including:
- The anticipation of the need for resuscitation: In this new guideline, the AHA and ILCOR state that at least one provider skilled in newborn resuscitation should attend every birth to provide immediate care to the newborn when needed.5
- Temperature management of the newborn: The guidelines recommend placing a newborn in skin-to-skin contact with the mother as long as the infant does not require resuscitation. That simple procedure can help maintain a normal temperature and provide other benefits to the newborn.
- Airway clearing in the presence of meconium: The updated guidelines indicate that newborns with apnea or ineffective breathing following delivery through meconium-stained amniotic fluid should not be treated with routine laryngoscopy for suctioning. However, if airway obstruction is evident, intubation and tracheal suctioning may be indicated.
- Preferred vascular access: When a newborn requires vascular access, the umbilical vein should be the preferred route of vascular access. If IV access is not available, the IO route can be used.
- Resuscitation termination: After all resuscitation steps are completed without the return of a viable heartbeat within 20 minutes, the team should discuss the termination of resuscitation with the family. These newborns are not likely to survive.
- Newborn resuscitation training: Training for individuals responsible for newborn resuscitation should occur more frequently than every two years to maintain knowledge and skills.
Resuscitation Education Science
The 2020 update stresses the importance of continuing resuscitative education, including:
- Deliberate practice in basic and advanced life support skills: The guidelines recommend incorporating education that promotes deliberate practice to improve mastery of basic and advanced life support.
- Supplement mass learning with booster and spaced learning sessions: In addition to mass learning of basic and life support, the guidelines recommend adding brief booster sessions to reinforce learning. The guidelines also recommend considering spaced learning sessions to replace traditional mass learning events for basic and advanced life support.
- Combine self-instruction and instructor-led instruction with hands-on training if available: When instructor-led training is not available, the guidelines recommend using a combination of instructor-led and self-instruction learning with hands-on training.
- In situ education: This new recommendation states that simulation-based training in patient care can supplement or replace traditional training.
- Training for high school and middle school students in CPR: This new recommendation is to train middle and high school students in performing CPR.
- Use virtual reality and games for basic and advanced life support training for lay and trained rescuers: This new recommendation states that trainers can consider using games and virtual reality to train both lay rescuers and healthcare rescuers in BLS and ACLS.6
- Train lay rescuers in opioid overdose training: This new recommendation proposes that lay rescuers should receive training in opioid overdose, including the administration of naloxone.
- Target training for lay rescuers in underserved socioeconomic communities: This new guideline recommends training lay rescuers in CPR in low-income or underserved communities.
- Reinforce the need for bystanders to perform CPR on women: Many bystanders hesitate to provide CPR to women resulting in poor outcomes for women. In this guideline, the recommendation is to address the reasons for this hesitancy through public education.
- EMS systems must monitor EMS personnel in providing resuscitation: This new guideline recommends that EMS systems monitor the competency of their staff to improve the care provided for cardiac arrest patients.
- Healthcare professionals should take an adult ACLS course: This new guideline states that it may be reasonable for all healthcare professionals to take an ACLS or equivalent course.
- Reinforce the need for bystanders to perform CPR: This guideline states that communities may provide CPR training and awareness initiatives to improve lay rescuers’ willingness to perform CPR. Hands-only CPR should be emphasized for lay rescuers.
Systems of Care
The 2020 update stresses the importance of Systems of Care that should include the lay public, trained responders, EMS systems, in-hospital nurses, physicians, professional support personnel, and the external companies that provide medications, equipment, and instructors, and others. To this end, the 2020 update includes the following recommendations:
- Use of mobile phones to alert bystanders of a nearby event: The guidelines recommend using mobile phone technology to alert bystanders that an emergency is in process near them.7 That would allow early assistance for a lone provider at the scene. Although not generally available in the United States, this technology could decrease the time to definitive therapy.
- Collection of data by organizations providing care for cardiac arrest patients: Registries provide local, state, and national collection of data to improve patient care and outcomes.