Introduction to ACLS Drugs
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- This is a quick introduction to medications used in ACLS.
- Clinicians will learn each drug’s mechanism of action, indications, dosing, and special considerations.
- Clinicians must know when and how to administer each drug to optimally treat patients.
The Role of Medications in ACLS Interventions
Let’s review the medications used in Advanced Cardiovascular Life Support (ACLS) during a cardiac arrest and other severe cardiovascular emergencies. Whether you are completing an ACLS certification online program, attending in-person training, or preparing for ACLS recertification online, it is essential to understand each medication’s pharmacology, indications, dosing, and special considerations. This knowledge is critical for safe and effective care. These concepts and skills can also be reinforced through the use of ACLS simulators. For medications, we will be reviewing:
- Pharmacology
- Indications
- Dosing
- Special considerations
Let’s start by looking at the pharmacology of the drug. What is its mechanism of action? How is it working inside the patient?
Next, we’ll look at the indications. That’s the reason why we’re giving the drug. What condition are we administering this medication for? As you can imagine, the same drug can have multiple indications of use.
The indication of the drug refers to the use of the drug.
Finally, we’ll examine some special considerations for the medications. One consideration is safety. Performing a task “the wrong way” can be dangerous, unprofessional, and life-threatening. Performing a task the right way should be efficient, safe, and meets the industry standards.
ACLS Medication Safety and Error Prevention
Case Study: A Near-Miss Medication Error
Last weekend, I was flying a cardiac patient up to Canada. The patient came down to visit family here in America, got sick and wound up on an intra-aortic balloon pump. We had to fly this patient back to Canada.
Now, before we loaded her up and took off from the ICU, I wanted to give her a little Zofran (ondansetron). Zofran is an antiemetic, or an anti-nausea medication. It has relatively low side effects and is a pretty safe drug.
Medication Error Prevention Checklist
- Right patient, right drug, right dose, right route, right time (pause and confirm before pushing).
- Use a second-person verification for IV push meds whenever possible.
- Read the label out loud (drug + concentration) before drawing up and again before administration.
- Standardize code meds: pre-labeled syringes, consistent concentrations, and organized code carts.
- Clarify look-alike/sound-alike medications and separate storage.
- Document dose/time immediately; assign a team member to closed-loop medication communication.
Why this matters: medication errors are a major patient-safety issue worldwide and are a key reason ACLS teams emphasize verification, labeling, and closed-loop communication.
If you can, get a second set of eyes prior to administering the drug to help prevent medication errors.
So, I’m at the counter in the ICU. I pull out the Zofran and I look at it. I turn to the ICU nurse behind the counter and I say, “This is Zofran.”
She looks up and she says, “That is Zofran” and goes back to work.
That is the height of professionalism and the height of patient safety. Why did I verify that drug? Because every year thousands of patients die from medication errors that we cause. One way I try to minimize that is to get a second set of eyes on every drug before I administer it. We’re talking about ACLS emergencies. That’s when accidents happen, right? You go into a code in the hospital and things get hectic. You could easily give the wrong medication.
Medication errors can also occur due to complacency, like giving a seemingly plain drug like Zofran. Check your medications. We’ll dive into the ACLS medications in the next few articles.
Read: General Stroke Care
Epinephrine in Cardiac Arrest: Timing, Dosing, and Controversy
What it does (pharmacology): Epinephrine stimulates alpha- and beta-adrenergic receptors. In cardiac arrest, the alpha-1 vasoconstriction effect is key because it increases aortic diastolic pressure and improves coronary and cerebral perfusion during CPR.
Indications in ACLS: Epinephrine is used in adult cardiac arrest for shockable rhythms (VF/pVT) and non-shockable rhythms (asystole/PEA), as part of the standard ACLS algorithm.
Standard adult dosing: 1 mg IV/IO every 3–5 minutes during cardiac arrest.
Timing pearls (high yield):
- Non-shockable (PEA/asystole): give epinephrine as soon as feasible, while continuing high-quality CPR.
- Shockable (VF/pVT): prioritize early defibrillation and CPR; epinephrine is typically introduced after initial shocks/CPR cycles per ACLS workflow.
Why it’s debated: Large trials and guideline discussions note that epinephrine increases ROSC and survival, but some evidence shows survivors may have a higher burden of severe neurologic impairment, so teams still follow ACLS algorithms while emphasizing early defibrillation (when indicated) and excellent CPR as the foundations of outcome.
Clinical pearls:
- Flush well after IV push and resume CPR immediately—don’t pause compressions for drug delivery.
- If using an IV in a small peripheral line, ensure the drug reaches central circulation (flush + elevation when appropriate).
- Track dose/time with a dedicated recorder using closed-loop communication.
Amiodarone and Lidocaine: Rhythm-Specific Antiarrhythmics
Amiodarone and lidocaine are commonly used in ACLS for refractory VF/pulseless VT after defibrillation attempts and ongoing CPR.
Amiodarone
- Typical use: VF/pVT that persists after shocks + CPR.
- Dose (adult): 300 mg IV/IO bolus; may give an additional 150 mg if needed.
- Key considerations: follow with a flush; continue CPR immediately; watch for hypotension/bradycardia in post-ROSC care.
Lidocaine
- Typical use: Alternative to amiodarone for VF/pVT; may be preferred in some systems based on availability/protocol.
- Dose (adult): 1–1.5 mg/kg IV/IO; may repeat 0.5–0.75 mg/kg, up to a maximum of 3 mg/kg.
- Key considerations: dose carefully in older adults or hepatic dysfunction; monitor for neurologic toxicity in post-ROSC settings.
Quick comparison
- Both are used for refractory VF/pVT in ACLS.
- Amiodarone is commonly taught as first-line antiarrhythmic for refractory VF/pVT, with lidocaine as an accepted alternative depending on protocol.
Magnesium Sulfate
When to think magnesium: Magnesium sulfate is most associated with treatment of Torsades de Pointes (a polymorphic VT typically linked to a prolonged QT interval). Torsades often appears as a “twisting” polymorphic wide-complex tachycardia.
Common ACLS dosing (adult): 1–2 g IV/IO diluted in 10 mL D5W, given over 5–20 minutes. In unstable torsades or cardiac arrest, protocols may administer magnesium more rapidly per local guidance.
Administration tips:
- Correct contributing factors: stop QT-prolonging drugs, treat hypokalemia/hypomagnesemia, and manage bradycardia when relevant.
- Continue rhythm reassessment and be ready for defibrillation if the rhythm becomes VF/pVT.
Practical Considerations for Drug Administration in ACLS
- High-quality CPR first: medications support resuscitation, but compressions/defibrillation (when indicated) drive outcomes.
- Use IV/IO correctly: IV is preferred when readily available; IO is fast and effective when IV access is delayed.
- Flush and resume compressions: after IV push meds, flush and immediately continue CPR—avoid interruptions.
- Closed-loop communication: the medication administrator repeats the order, dose, and time; the recorder confirms documentation.
- Standardize concentrations: avoid calculation errors during codes by using standard prefilled syringes and labels.
- Post-ROSC transition: re-check blood pressure, oxygenation and carbon dioxide ventilation parameters, ECG, glucose, and temperature goals; reassess the need for antiarrhythmics and pressors.
Summary
ACLS medications work best when paired with the fundamentals: high-quality CPR, early defibrillation when indicated, and coordinated team performance. In cardiac arrest, epinephrine is administered as part of the ACLS algorithm, while rhythm-specific antiarrhythmics (such as amiodarone or lidocaine for refractory VF/pVT) and magnesium sulfate (for torsades de pointes) are used when clinically appropriate. Finally, medication safety practices verification, labeling, closed-loop communication, and standardized processes help prevent errors during high-stress resuscitations.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
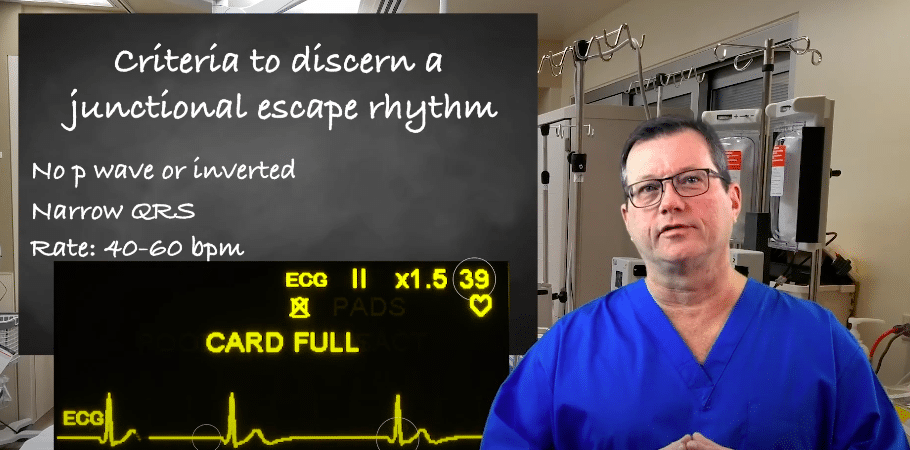
Learn about junctional escape rhythm criteria for ACLS certification with our article. Understand the guidelines and requirements seamlessly.
Understand basic life-saving skills and how BLS classes vary based on experience levels. Our article offers insights from a lay person's perspective to that of a licensed professional.