Ultimate Guide to ACLS Algorithms: Cardiac Arrest
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- In both pulseless electrical activity (PEA) and asystole, the patient does not have a pulse.
- Ventricular fibrillation (VF) and pulseless ventricular tachycardia (PVT) are conditions categorized by rapid, disorganized electrical activity in the patient’s heart.
- Providers will learn the ACLS algorithms for a lifeless patient.
Advanced Cardiovascular Life Support Algorithms
Advanced Cardiovascular Life Support (ACLS) algorithms are broken into two major categories:
- Dead patient algorithms
- Alive patient algorithms
This lesson only discusses lifeless patient algorithms. It examines pulseless electrical activity (PEA) and asystole, which are treated the same way, before moving on to ventricular fibrillation (VF) and pulseless ventricular tachycardia (PVT).

Adult Cardiac Arrest Algorithm
Steps for Treating PEA and Asystole
A clinician practices the following steps when treating PEA and asystole:
- Start cardiopulmonary resuscitation (CPR)
- Ensure IV/monitor/O2 are administered and monitored
- Check the heart’s rhythm
- Administer epinephrine
- Perform CPR and consider advanced airway

Asystole presents as a flatline on the electrocardiogram (EKG). There is no pulse.
1) Cardiopulmonary Resuscitation
A patient experiencing PEA is conducting electrical activity through their heart, but it isn’t sufficient to generate a pulse. The patient is dead. Asystole is a heart rhythm with no discernable electrical activity.
Clinicians will always start their algorithms with high-quality cardiopulmonary resuscitation (CPR), as outlined in the adult cardiac arrest algorithm, beginning with high-quality chest compressions at a rate of at least 100 to 120 compressions per minute, a skill reinforced during the ACLS renewal course online. An easy mnemonic device to remember is the song “Another One Bites the Dust.” If a provider compresses to the beat, their pace is adequate.
Providers should also pay attention to compression depth, making sure each compression is two inches deep accompanied by full chest recoil. If time and resources are available, use arterial blood pressure and ETCO2 to monitor the quality of CPR.
Related Video – Understanding the Adult Cardiac Arrest Algorithm

Chest compressions need to be fast and deep.
2) Connect Patient to the Monitor, Set Up the IV, and Take Care of Oxygen
Next, the clinician attaches the monitor and provides the patient with oxygen (O2). If a provider suspects a cervical spine injury, they perform the head-tilt chin-lift maneuver or the jaw thrust. They will also bag the patient with a bag-mask (Ambu bag).
The ratio of chest compressions to breaths is 30 to 2. The clinician will ensure the IV is set up for medication administration. ILCOR recommends IV over IO access during cardiac arrest.
3) Check Rhythm
After two minutes or five cycles of CPR, the clinician checks for a heart rhythm on the monitor as well as the pulse at the carotid. The provider should never check for a pulse for no longer than 10 seconds to avoid any sustained compression interruption. If the patient is pregnant, follow the Cardiac arrest in pregnancy — In‑Hospital ACLS algorithm when transitioning to advanced care to ensure pregnancy‑specific airway, positioning, and team role adjustments are made without delay.
A patient with PEA or asystole with no pulse is not shockable.
In this case, the algorithm suggests medication intervention while continuing CPR.
4) Administer Epinephrine
The drug of choice during CPR is 1 mg epinephrine administered through IV every three to five minutes at a concentration of 1:10,000.
Clinicians need to provide at least 20 ml of a flush. If it’s in a peripheral IV, elevate the arm because the patient is technically deceased. If the arm isn’t lifted, allowing gravity to work the drug down to the patient’s heart, the epinephrine won’t circulate.
Related Video – Epinephrine – ACLS Drugs
5) Consider an Advanced Airway
Following epinephrine and CPR, providers should consider an advanced airway, or intubation.
Once the patient is intubated, breath to chest compression ratio no longer exists. The administering clinician will compress at least 100 to 120 times a minute, and the clinician delivering breaths will give a breath every 6 seconds. Once the patient is intubated the provider no longer pause chest compressions.
Read: VF and PVT: Care of the Patient with a Shockable Rhythm
Consider Reversible Causes
A clinician should also consider the Hs and Ts, otherwise known as reversible causes of cardiac arrest. For example, a common cause of asystole or PEA is pulmonary embolus (PE).
Related Video – One Quick Question: What are Hs and Ts?
The Hs and Ts to assess are:
Hs:
- Hypovolemia
Related Video – Hs and Ts – Hypovolemia
- Hypoxia
Related Video – Hs and Ts – Hypoxia
- Hydrogen ion (acidosis)
Related Video – Hs and Ts – Hydrogen Ions
- Hyper/hypokalemia
Related Video – Hs and Ts – Hypo-Hyper Kalemia
- Hypothermia
Related Video – Hs and Ts – Hypothermia
- Note: Hypoglycemia used to be in the Hs and has since been removed. It is still considered important during a cardiac arrest assessment.
Ts:
- Toxins
Related Video – Hs and Ts – Toxins
- Tamponade (cardiac)
Related Video – Hs and Ts – Cardiac Tamponade
- Tension pneumothorax
Related Video – Hs and Ts – Tension Pneumothorax
- Thrombosis (coronary and pulmonary)
Related Video – Hs and Ts – Pulmonary Embolism
- Note: Trauma used to be in the T’s and has since been removed. It is still considered important during a cardiac arrest assessment.
Hyper and hypokalemia are sometimes side effects of patients undergoing dialysis who miss a treatment, resulting in elevated or lowered potassium levels. With hypovolemia, the provider needs to watch for hypovolemic shock. For hypothermia, warming measures should be taken if the patient was exposed to the cold.
Toxins are usually due to drug overdoses that cause pulseless arrest.
Pulmonary thrombosis may be exhibited through a pulmonary embolism, which blocks the arteries to the lungs and can contribute to respiratory failure, obstructive shock, or cardiac arrest.
Coronary thrombosis causes myocardial infarction or heart attack, which destroys heart muscle and leads to respiratory arrest.
The following videos are steps a clinician should take to treat PEA and asystole. They will repeat these steps until the patient is recovered.
Related Video – What is PEA?
Related Video – Hs and Ts – Treating Asystole
Related Video – ECG Rhythm Review – Asystole
Steps for VF and Pulseless VT
Providers need to make sure not to confuse pulseless VT with VT with a pulse. If the patient has a pulse, do not start CPR, as these distinctions are covered in basic arrhythmia certification programs. If they’re pulseless, the provider should begin CPR.
Related Video – ECG Rhythm Review – Ventricular Tachycardia
1) Start with High-quality CPR
Just like with asystole and PEA, providers start with high-quality CPR. The chest compression-to-breath ratio is 30 to 2.
Related Video – CPR for Adults with 2 Rescuers
2) Connect Patient to the Monitor, Set Up the IV, and Take Care of Oxygen
Make sure the monitor is attached as well as the defibrillation pads. Ensure the patient’s O2 is taken care of by making sure they’re bagged with a good chest rise and fall. Clinicians should also insert an IV.
3) Check the Rhythm
The provider must check the patient’s rhythm on the monitor and via a pulse after the first two minutes of CPR. If the patient has VF or pulseless VT, the provider will administer shock via defibrillation. For a quick review of how chest compressions and shocks work together, see CPR vs defibrillation.
4) Shock the Patient
Clinicians will deliver stacked shocks. The first shock is at 120 joules, assuming it is performed with a biphasic defibrillator. Biphasic means electricity is given in two directions. One pad is placed on the front and one in the back. Biphasic defibrillators are generally the hospital standard.

To reset the heart rhythm, the defibrillator machine generates electricity.
5) Perform CPR Immediately After Shocking the Patient
Immediately after the shock, a provider resumes high-quality CPR again for two more minutes or five more cycles.
6) Check Rhythm Again and Determine if Patient is Shockable
After two minutes or five cycles of CPR, the provider checks for a pulse again. If the patient still has VF or pulseless VT, shock them again.
7) Shock at 150 Joules
If a pulse is present, shock the patient at 150 joules. In a stacked shock, the joules get higher with each shock. The clinician immediately resumes CPR and chest compressions after the second shock.
At this point, the provider should consider drugs. If the rhythm is shockable, the provider will always shock twice before considering drugs. In patients with asystole and PEA, the provider immediately starts giving drugs after the first two-minute round of CPR.
8) Consider Epinephrine after Shocking the Patient Twice
Epinephrine is the first drug a provider considers. Give 1 mg of 1:10,000 epinephrine. Make sure to elevate the patient’s arm to circulate the medication.
Epinephrine is proven to improve a patient’s response to the shocks. While a clinician is attempting to improve contractility and rate, they’re also trying to improve the patient’s defibrillation responsiveness.
9) Shock at 200 Joules
A clinician may shock a patient again after two more minutes of CPR or five more rounds. If the patient is rhythm shockable, the third pulse is 200 joules. It is the maximum amount a physician will deliver during defibrillation with a biphasic defibrillator.
Consider Hs and Ts
A provider must consider the Hs and Ts. A patient with VF or PVT has a higher survivability than one with asystole and PEA. Patients with asystole and PEA have no heart activity and poor outcomes, so it’s important to consider reversible causes.
Providers should still consider Hs and Ts with VF and VT, but when a patient goes into VF or PVT, it’s usually an MI. Consider coronary thrombosis in these cases.
Related Video – Understanding the Adult Cardiac Arrest Algorithm
Summary
If a patient exhibits cardiac symptoms of PEA or asystole, they don’t have a discernible pulse. A clinician should start CPR, ensure airways are open, check cardiac rhythm, and administer epinephrine as soon as possible.
If a patient is experiencing VF or PVT, their cardiac activity is rapid and disorganized. A pulse is not palpable and cardiac output is absent. A clinician should start CPR, ensure airways are open, check cardiac rhythms, and then deliver a shock via defibrillation as soon as possible, followed by an additional shock every 2 minutes if the shockable rhythm persists. In all cases of asystole, PEA, PVT, or VF, providers should check for reversible causes, Hs and Ts.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
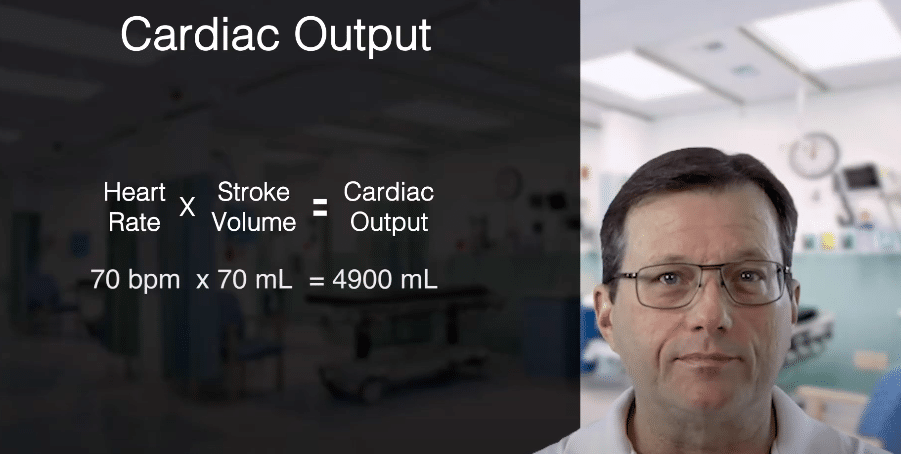
Master the cardiac output formula with our ACLS certification guidelines. Our article will help you learn to calculate cardiac output accurately and effectively.
Uncover the potential of Adenosine Injection in ACLS drug therapy for SVT. Our article details proper dosing and administration for effective life-saving interventions.