Hypovolemia: Symptoms, Causes, and Treatment (ACLS Hs & Ts)
Hypovolemia is a life-threatening decrease in blood volume that can rapidly lead to cardiac arrest if left untreated. Designed for ACLS learners and clinical providers, this guide explores the critical signs, underlying causes, and evidence-based treatments for this condition. By the end of this article, you will be able to confidently recognize hypovolemia, understand its progression to pulseless electrical activity (PEA), and implement immediate resuscitative interventions.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Hypovolemia is one of the Hs and Ts (a mnemonic for the reversible causes of cardiac arrest) and a reversible cause of cardiac arrest.
- It is usually caused by blood loss but may be caused by nausea, vomiting, or other fluid loss.
- Signs and symptoms include tachycardia, peripheral shutdown (a massive diversion of blood away from the extremities to preserve core organs), and clammy and pale skin.
- Hypovolemia is often associated with PEA (Pulseless Electrical Activity).
- To treat hypovolemia, the provider should administer fluid or blood.
Hypovolemia
Hypovolemia is defined as a significant decrease in the blood volume circulating in the body. This critical reduction generally stems from two main categories: severe fluid loss (dehydration) or direct bleeding (hemorrhage). Recognizing this condition early is paramount, as an untreated hypovolemic patient can rapidly progress to severe shock, arrest, and death.
What is hypovolemic shock?
While hypovolemia refers strictly to the loss of volume, hypovolemic shock occurs when that volume loss becomes so severe that the heart is unable to pump enough blood to effectively oxygenate the body’s vital organs. You can learn more about how it compares to other critical states in our comprehensive guide on the types of shock.
What are the symptoms of hypovolemia?
Symptoms progress as the body loses more volume. Clinicians should monitor for both early warning signs and severe ACLS-relevant indicators:
- Mild to Moderate: Thirst, dry mucous membranes, fatigue, dizziness, and decreased urine output.
- Severe (Approaching Arrest): Tachycardia, tachypnea, clammy and pale skin, profound hypotension (dangerously low blood pressure), confusion, and peripheral shutdown.
Two Main Causes of Hypovolemia
Hypovolemia is broadly driven by either the loss of body fluid (such as water and electrolytes) or the direct loss of whole blood. Understanding which mechanism is causing the volume deficit is critical for selecting the correct resuscitative intervention.
Hypovolemia Through Fluid Loss
What causes hypovolemia in the context of fluid loss?
Non-hemorrhagic volume depletion usually results from severe fluid and electrolyte loss. Common triggers include:
- Excessive vomiting
- Severe diarrhea
- Profound sweating
- High fever
To understand fluid loss, you need to think about the body’s compensatory mechanisms. What’s going to happen in the body during fluid loss?
Tachycardia
The heart rate is going to increase in an attempt to maintain cardiac output. Therefore, your patient might be very tachycardic.
Vasoconstriction and Peripheral Shutdown
The other mechanism to raise blood pressure is peripheral vasoconstriction. This causes “peripheral shutdown,” a massive diversion of blood away from the limbs and skin to prioritize the brain and core organs.
Vascular Access Difficulties
Because of this shutdown, it might be very difficult to get an IV in your patient. You may need to take the intraosseous (IO) route. Note that timing is protocol-dependent; however, a common standard suggests moving to IO access if an IV cannot be established after two attempts or 90 seconds (per AHA guidelines).
If intravenous (IV) route fails, then you will proceed to intraosseous (IO).
Mean Arterial Pressure (MAP)
Evaluating perfusion during fluid loss relies heavily on monitoring Mean Arterial Pressure (MAP). Providers use the MAP in other formulas to calculate other pressures throughout the body. It is also used as a guideline in certain treatment algorithms, such as the sepsis algorithm.
Read: ACLS Hs & Ts – Cardiac Tamponade
Hypovolemia Through Blood Loss
What causes hypovolemia in the context of hemorrhage?
Another type of volume loss is blood loss. It can stem from:
- External Bleeding: Visible trauma, massive lacerations, or surgical complications.
- Internal (Occult) Bleeding: Severe internal bleeding such as GI bleeds, ruptured aortic aneurysms, or ectopic pregnancies.
With blood loss, a confounding factor is that oxygen-carrying capacity is also lost due to less hemoglobin. The reason hypovolemia made its way to the Hs and Ts list is because hypovolemia is often associated with pulseless electrical activity (PEA ACLS), a rhythm where the heart may contract but cardiac output is insufficient to generate a pulse.
Related Resource: The video below provides a comprehensive breakdown of Pulseless Electrical Activity (PEA). It visually explains why electrical signals may still appear on a monitor even when mechanical pumping fails to produce a pulse, making it crucial for understanding hypovolemic cardiac arrest.
Case Callout: Recognizing Occult Bleeding and Arrest
- Recognition Clues: Notice the patient’s skin—it is often very pale. Current guidelines emphasize looking for occult bleeding (bleeding that you can’t see because it’s occurring on the inside).
- Source Considerations: In some cases, such as bright red blood around an endotracheal tube, the source could be esophageal varices or a ruptured gastric ulcer.
- ACLS Progression: No matter the source, profound blood loss can quickly escalate. The patient may initially be very tachycardic, but shortly after, they can arrest and develop PEA.
This patient is experiencing hypovolemia and PEA.
How do you know the heart is working in PEA?
So how do you know if the heart is even working?
- Auscultation: If the valves are opening and closing, you’ll have heart tones. If you can’t feel a pulse, you might still be able to hear the heart.
- Doppler: You could pull out a Doppler and try to find pulses.
- Ultrasound: You can also perform a bedside echo. Look at the contractions to see if the heart is physically moving or not.
Use a doppler to find any heart tones.
Treatment of Hypovolemia
Successful resuscitation depends heavily on targeting the specific type of volume deficit.
- For Non-Hemorrhagic Fluid Loss:
- Replace the deficit with a crystalloid solution, typically 0.9% normal saline.
- Follow your local protocols for dosing. Many AHA guidelines recommend an initial rapid fluid bolus of 500 mL to 1 liter for adults, though some protocols call for 200 mL depending on the patient’s condition.
(Note: Pediatric fluid resuscitation doses differ significantly from adults; comprehensive training can be found in a PALs Certification course.)
- For Hemorrhagic Shock (Blood Loss):
- To treat hypovolemia and reverse hemorrhagic shock caused by blood loss, replace the lost blood. Activate your massive transfusion protocol if indicated by your facility’s guidelines.
- Control the source of bleeding immediately (e.g., tourniquets, surgical intervention).
- Reassessment:
- Continuously evaluate the patient’s MAP, heart rate, and perfusion status.
- Caution: Any time you’re rapidly putting fluid into a patient, you want to continuously monitor their lungs for signs of fluid overload.
Related Resource: Once you have identified PEA or asystole, rapidly treating the underlying reversible cause (such as hypovolemia) is your top priority. This video outlines the algorithm and actionable steps for addressing the Hs and Ts during an active code.
Frequently Asked Questions
What tests diagnose hypovolemia?
Diagnosis primarily relies on clinical signs (tachycardia, hypotension, pale skin), but can be supported by labs like lactate levels, hemoglobin/hematocrit (for bleeding), and bedside ultrasound to assess cardiac contractility and inferior vena cava (IVC) variability.
What are the potential complications of hypovolemia?
If not rapidly reversed, hypovolemia progresses to hypovolemic shock, leading to inadequate tissue perfusion, multi-organ failure, pulseless electrical activity (PEA), and death.
What is the difference between hypovolemia and hypervolemia?
Hypovolemia refers to a dangerous decrease in blood volume (due to fluid or blood loss), whereas hypervolemia is an excess of fluid volume in the body, often leading to swelling and fluid accumulation in the lungs (pulmonary edema).
Summary
How you treat hypovolemia depends on its cause. For fluid loss, replace with normal saline. For blood loss, replace it with blood. Remember, hypovolemia often causes PEA. For that reason, it is one of the Hs and Ts. However, the most crucial takeaway is the importance of early recognition and continuous reassessment: swiftly identifying signs of peripheral shutdown and promptly troubleshooting PEA can make the difference between a reversible event and a fatal cardiac arrest.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
Read our detailed article and watch the video on Hyper vs. Hypothyroidism. Understand the etiology, the pathophysiology, and the unique...
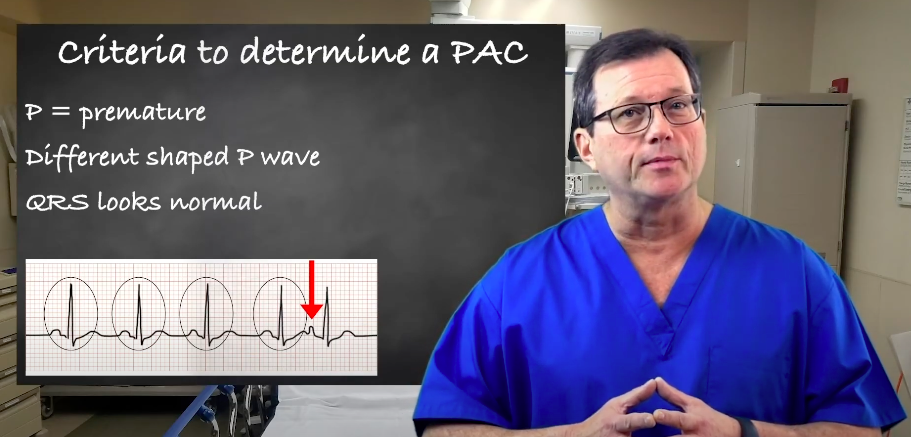
Explore premature atrial contractions (PACs) and the three determinants used to identify them. Our article will enhance your understanding of cardiac arrhythmias.