Hs & Ts – Pulmonary Thrombosis
This ACLS Hs and Ts lesson is for students, clinicians, and resuscitation-team members reviewing pulmonary thrombosis as a reversible cause of cardiac arrest. It explains the terminology, risk factors, clinical presentation, diagnosis, and treatment priorities for pulmonary embolism in the emergency and ACLS context.
Strictly speaking, pulmonary thrombosis means clot formation within the pulmonary circulation, while pulmonary embolism means a clot or other embolic material travels to the pulmonary arteries from another location. In ACLS Hs and Ts teaching, “pulmonary thrombosis” commonly refers to embolic pulmonary embolism (PE), and this lesson focuses on that embolic PE scenario.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Pulmonary thrombosis is one of the ACLS Hs and Ts and is commonly taught in the context of pulmonary embolism as a reversible cause of cardiac arrest.
- Pulmonary embolism occurs when embolic material blocks pulmonary blood flow, most often after a clot forms in a deep vein and travels to the lungs.
- PE can create ventilation/perfusion mismatch because parts of the lung may still receive air but have reduced or absent blood flow.
- Risk assessment should be category-based, including prior clots, immobility, surgery, cancer, pregnancy/postpartum status, estrogen therapy, thrombophilia, smoking, and obesity.
- Treatment depends on severity and bleeding risk, and may include anticoagulation, thrombolysis in select unstable cases, catheter-based therapy, surgical embolectomy, or supportive care during resuscitation.
What is a Pulmonary Embolism?
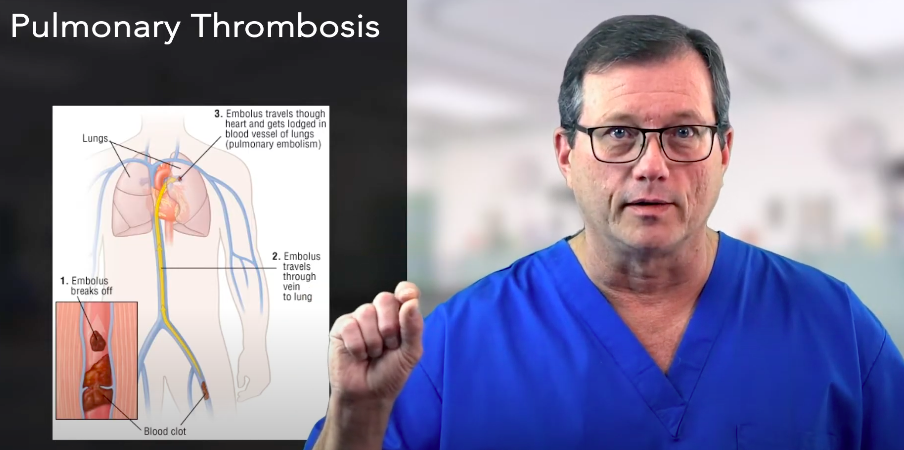
A pulmonary embolism (PE) is a blockage in a pulmonary artery that reduces blood flow through part of the lung. In most cases, the blockage is a blood clot that forms elsewhere in the venous system, breaks free, travels through the right side of the heart, and lodges in the pulmonary circulation.
In the ACLS Hs and Ts framework, pulmonary thrombosis is treated as a potentially reversible cause of cardiac arrest, and this lesson focuses on embolic pulmonary embolism pe rather than every possible cause of pulmonary artery obstruction. Non-clot emboli, such as air, fat, or amniotic fluid, can occur but are less common and are outside the main scope of this lesson.
A pulmonary embolism often begins as deep vein thrombosis in a leg or pelvic vein. The clot can travel through the inferior vena cava, into the right atrium, through the right ventricle, and out through the pulmonary artery.
What are signs and symptoms of Deep Vein Thrombosis (DVT)?
- Swelling in one leg or arm
- Pain or tenderness, often in the calf or thigh
- Warmth over the affected area
- Redness or skin discoloration
- New or unexplained leg symptoms in a patient with PE risk factors
When the embolus blocks pulmonary blood flow, the affected area may still receive air but may not receive enough blood for gas exchange. This creates a ventilation/perfusion mismatch, often abbreviated V/Q mismatch.
Key terms
- Thrombus: a blood clot that forms inside a blood vessel.
- Embolus: material, often a clot, that travels through the bloodstream and lodges somewhere else.
- Thrombosis: the process of clot formation inside a vessel.
- Embolism: blockage caused by an embolus lodging in a blood vessel.
- V/Q mismatch: ventilation and perfusion are not matched, meaning air reaches part of the lung but blood flow is reduced or absent.
An embolus is a clot or other material that travels through the body and lodges in another vessel.
What are Hypoxia Shunts?
This video explains how abnormal oxygenation can occur when ventilation and perfusion are not matched. It fits here because pulmonary embolism can create areas of the lung that are ventilated but poorly perfused.
Severity and outcomes
The severity of acute pulmonary embolism depends on more than clot size alone. Hemodynamic effects, right ventricular strain, oxygenation, comorbid disease, and whether the patient develops hypotension or cardiac arrest all affect risk. Because the current page does not provide a source for the specific cardiac arrest and mortality percentages, I recommend removing those numbers rather than publishing unsupported statistics.
Risk Factors
Risk factors for pulmonary embolism should be presented by category rather than as one single “leading” cause. A patient’s risk often increases when more than one factor is present.
- History of clots: prior deep vein thrombosis, prior pulmonary embolism, or family history of venous thromboembolism.
- Immobility or hospitalization: prolonged bed rest, long travel, paralysis, or limited movement after illness or injury.
- Surgery or trauma: especially major abdominal, pelvic, hip, knee, or orthopedic surgery.
- Cancer and chronic illness: active cancer, cancer treatment, heart disease, lung disease, and inflammatory bowel disease.
- Pregnancy and postpartum status: risk can remain elevated after delivery.
- Estrogen exposure: estrogen-containing contraceptives or hormone therapy.
- Thrombophilia: inherited or acquired clotting tendencies.
- Modifiable risks: smoking, obesity, and prolonged sedentary behavior.
Risk factors for pulmonary embolism include immobility, surgery, smoking, obesity, estrogen exposure, pregnancy, cancer, and prior clots.
Can pulmonary embolism be prevented?
Prevention focuses on reducing venous thromboembolism risk when possible. Practical steps include early mobility after surgery or hospitalization, leg exercises during long travel, compression devices or stockings when recommended, prophylactic anticoagulation when prescribed, smoking cessation, and weight management.
Read: General Stroke Care
Symptoms and Clinical Presentation of Pulmonary Embolism
The clinical presentation of pulmonary embolism can vary from mild symptoms to obstructive shock or cardiac arrest. Symptoms do not reliably identify clot size, so suspected PE requires urgent assessment, especially when risk factors or DVT clues are present.
Common symptoms and signs may include:
- Sudden or unexplained shortness of breath
- Sharp or pleuritic chest pain that may worsen with deep breathing or coughing
- Tachycardia or palpitations
- Tachypnea or increased work of breathing
- Cough or hemoptysis
- Syncope, lightheadedness, or near-syncope
- Hypotension in severe cases
- Cyanosis, clammy skin, or signs of poor perfusion
- Unexplained anxiety or a sense of impending doom
- Leg swelling, pain, warmth, or redness as a clue to DVT
Diagnosis and Tests
Diagnosis of suspected pulmonary embolism is educationally best understood as a combination of pretest probability, symptoms, risk factors, physical findings, and selective testing. Clinicians choose tests based on how likely PE is and how stable the patient is.
Common evaluation steps and tests may include:
- Clinical assessment: history, vital signs, oxygenation, cardiopulmonary exam, and DVT symptom review.
- D-dimer: a blood test often used in lower-risk patients to help decide whether imaging is needed.
- CT pulmonary angiography (CTPA): a common imaging test used to identify clot burden in the pulmonary arteries.
- V/Q scan: a ventilation/perfusion scan that can help evaluate mismatch when CT contrast is not ideal or available.
- Leg ultrasound: used to identify deep vein thrombosis that may support the diagnosis.
- Echocardiogram: may help assess right ventricular strain in unstable or higher-risk patients.
- Chest X-ray: an adjunct test that may help evaluate other causes of chest pain or shortness of breath, but it does not rule out PE by itself.
This section is educational and not a diagnostic protocol. In actual care, test selection depends on local pathways, pretest probability, patient stability, contraindications, and clinician judgment.
Treatment
Treatment goals for pulmonary embolism are to support oxygenation and perfusion, prevent clot growth, reduce the risk of additional emboli, and restore circulation when PE causes shock or cardiac arrest.
- Anticoagulation: used for many confirmed or strongly suspected PE cases to prevent clot extension and new clot formation. Bleeding risk must be considered.
- Thrombolysis: may be considered in select high-risk or unstable PE cases when the potential benefit outweighs bleeding risk.
- Catheter-based therapy or thrombectomy: may be considered for selected patients with high-risk PE, persistent instability, or contraindications to thrombolytics.
- Surgical embolectomy: may be considered in severe cases when other therapies are not sufficient or not appropriate.
- Vena cava filter: other options exist for select patients, such as a vena cava filter when anticoagulation cannot be used or is not effective, but indications are specific and should follow specialist guidance.

Selected high-risk pulmonary embolisms may require catheter-based therapy, thrombectomy, or surgical embolectomy.
In the field
- Recognize possible PE based on sudden dyspnea, chest pain, tachycardia, hypoxia, hypotension, DVT clues, and risk factors.
- Support airway, breathing, circulation, and oxygenation according to scope and protocol.
- Alert the receiving hospital early when PE is suspected, especially if the patient is unstable.
- Prepare for obstructive shock or cardiac arrest if the patient deteriorates.
- Follow local ACLS and EMS protocols for resuscitation, oxygen, IV access, fluids, vasopressors, and transport decisions.
Hemodynamics in PE: hypotension and obstructive shock
Massive or high-risk PE can obstruct pulmonary blood flow, strain the right ventricle, reduce left-sided filling, and lower systemic blood pressure. Mean arterial pressure (MAP) can help describe perfusion pressure, but in suspected PE it should be interpreted with the full clinical picture, including mental status, oxygenation, pulse quality, skin signs, and shock severity.
Ventilation and Perfusion
This video explains how ventilation and perfusion work together to support gas exchange. It fits this treatment section because PE management often focuses on oxygenation, perfusion, and the consequences of V/Q mismatch.
Summary
Pulmonary thrombosis is one of the ACLS Hs and Ts, but this lesson focuses specifically on embolic pulmonary embolism. In most PE cases, a blood clot forms in the venous system, often as deep vein thrombosis, then travels through the heart to the pulmonary arteries.
Risk factors include prior venous thromboembolism, immobility, hospitalization, surgery, trauma, cancer, pregnancy or postpartum status, estrogen therapy, thrombophilia, smoking, and obesity. Symptoms can include sudden shortness of breath, pleuritic chest pain, tachycardia, tachypnea, hemoptysis, syncope, hypotension, cyanosis, anxiety, or leg findings that suggest DVT.
Diagnosis usually depends on pretest probability and selected testing such as D-dimer, CTPA, V/Q scan, leg ultrasound, echocardiography, and adjunct chest imaging. Treatment may include oxygen and hemodynamic support, anticoagulation, thrombolysis in select unstable cases, catheter-based therapy, thrombectomy, surgical embolectomy, or selective vena cava filter placement when appropriate.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
Determine whether the patient is "unstable in Tachycardia" if the initial interventions fail to correct the tachyarrhythmia. Read more in our detailed article.
Uncover the potential of Adenosine Injection in ACLS drug therapy for SVT. Our article details proper dosing and administration for effective life-saving interventions.