3rd Degree Heart Block: Criteria, Causes, and ECG Strip Interpretation
A 3rd degree heart block, also called complete heart block, is an AV conduction failure where P waves and QRS complexes occur independently. On ECG you will see AV dissociation with no consistent PR interval. This guide covers the criteria, step by step strip interpretation, common causes, symptoms, and treatment priorities including pacing decisions.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Table of Contents
- Third-degree Heart Block Criteria
- How to Identify a 3rd Degree Heart Block Strip
- ECG Strip Variations of Complete Heart Block
- Diagnosis vs. Criteria: How do clinicians confirm complete heart block?
- Common Causes of Complete (3rd Degree) Heart Block
- Clinical Signs and Symptoms
- Treatment Pathways for Third-Degree AV Block
- 3rd Degree Heart Block vs Mobitz II
- Frequently Asked Questions About 3rd Degree Heart Block
- Summary
What is a 3rd Degree Heart Block?
A 3rd degree heart block, also called complete heart block, occurs when atrial electrical impulses do not conduct through the AV node to the ventricles. The atria continue to follow the sinoatrial node, but the ventricles rely on a separate escape rhythm from a lower pacemaker site. This creates two independent rhythms on the ECG.
Why it happens: conduction tissue is blocked or damaged, so the ventricles activate independently. The escape rhythm may originate from the AV junction, producing a narrow QRS, or from the ventricles, producing a wide QRS. The defining feature remains AV dissociation with no consistent PR relationship.
This video gives a quick overview of AV blocks and how conduction problems progress. Watch the video to understand the basics before reviewing complete heart block criteria.
Article at a Glance
- Third-degree heart block is characterized by:
- Regularity: Regular
- Rate: Atrial rate 60–100 bpm; Ventricular rate depends on focus but usually 40–60 bpm
- P Wave: Uniform with more than one P wave for each QRS with no relationship
- PR Interval: No relationship to QRS so not measurable
- QRS Complex: If junctional focus, < 0.12 second; if ventricular focus, > 0.12 second
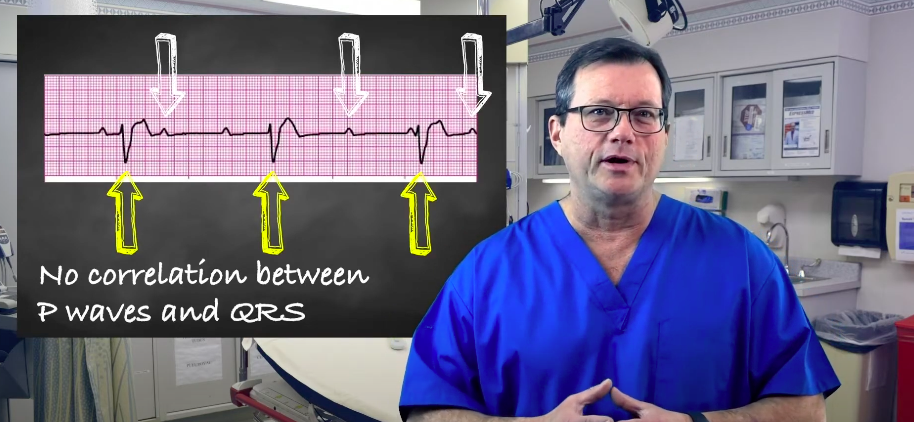
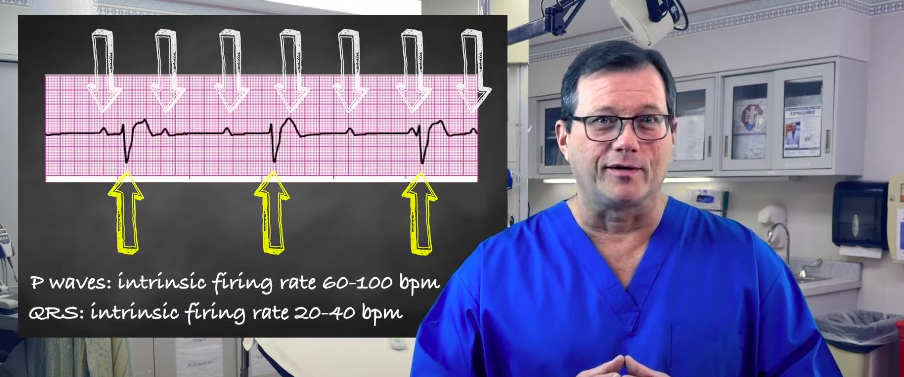
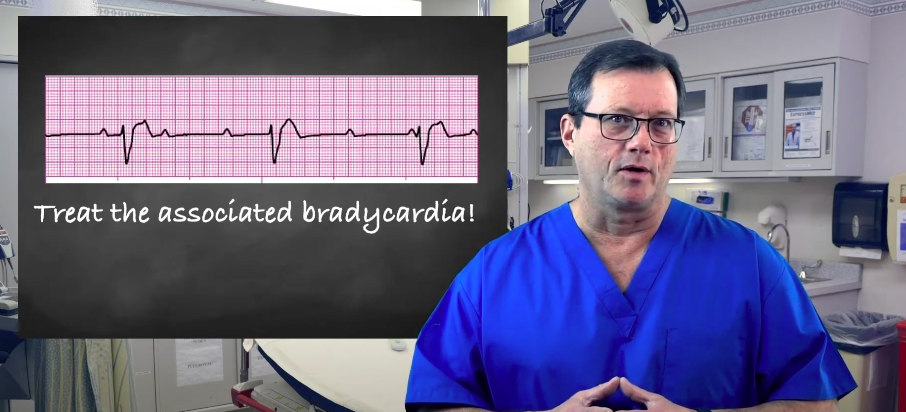
Physicians interpret an ECG tracing to discern potential third-degree or complete heart blocks. Accurate EKG interpretation is essential for recognizing this rhythm and distinguishing it from other arrhythmias such as SVT vs ST. You’ll first notice there is no correlation between the P waves and the QRS complex. The PR interval will either be missing or inconsistent, unlike a first degree heart block where the PR interval is consistently prolonged. In a third-degree heart block, there is no correlation between the P waves and the QRS complexes. The P waves march on their own, with an intrinsic firing rate (or heart rate) between 60 and 100 bpm. Similarly, the ventricular complexes and the QRS march out by themselves, typically within their own intrinsic firing rate between 20 and 40 bpm. Read: Criteria for a SVT (supraventricular tachycardia) The P waves and QRS typically occur at their respective intrinsic firing rates. Remember, we aren’t trying to match the P waves with the QRS or the atrial and ventricular contractions. If the ECG only displays the QRS as appearing 20–40 times, it’s a complete heart block. You must treat the underlying bradycardia. The treatment goal is to treat the associated bradycardia.Third-degree Heart Block Criteria
Related Video – ECG Rhythm Review – Third-Degree Heart Block?
How to Identify a 3rd Degree Heart Block Strip
ECG Strip Variations of Complete Heart Block
Complete heart block can look different depending on where the escape rhythm originates. The key feature is still AV dissociation with two independent marching rhythms.
Complete heart block strips can vary based on where the escape rhythm originates. A junctional escape often produces a narrow QRS and a slightly faster ventricular rate. A ventricular escape usually produces a wide QRS and a slower ventricular rate. Regardless of appearance, the defining feature is still AV dissociation: P waves march through at their own rhythm, and QRS complexes march through independently, with no repeating PR interval pattern.
- Variation 1: Narrow QRS junctional escape with AV dissociation
- Variation 2: Wide QRS ventricular escape with AV dissociation
- Variation 3: Independent atrial flutter activity with a separate escape rhythm
Variation 1: Regular P waves with a narrow complex junctional escape. Note AV dissociation and changing P wave position relative to QRS.
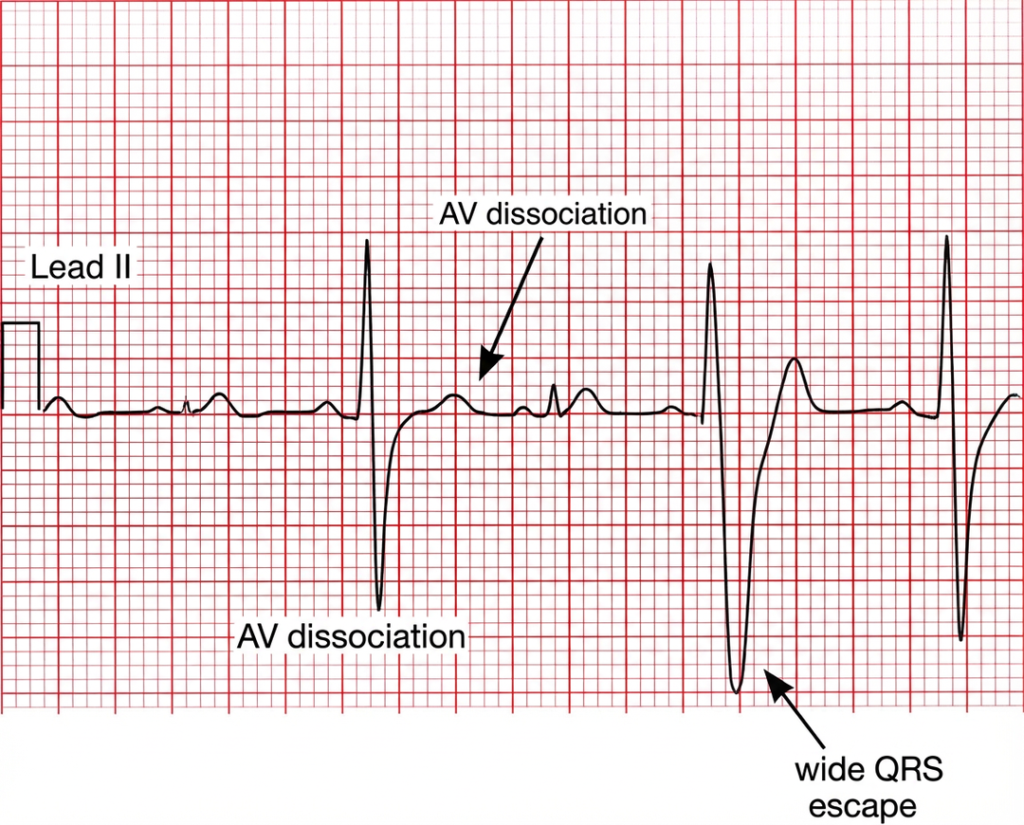
Variation 2: Complete heart block with a slow wide complex ventricular escape rhythm. P waves march through independently.
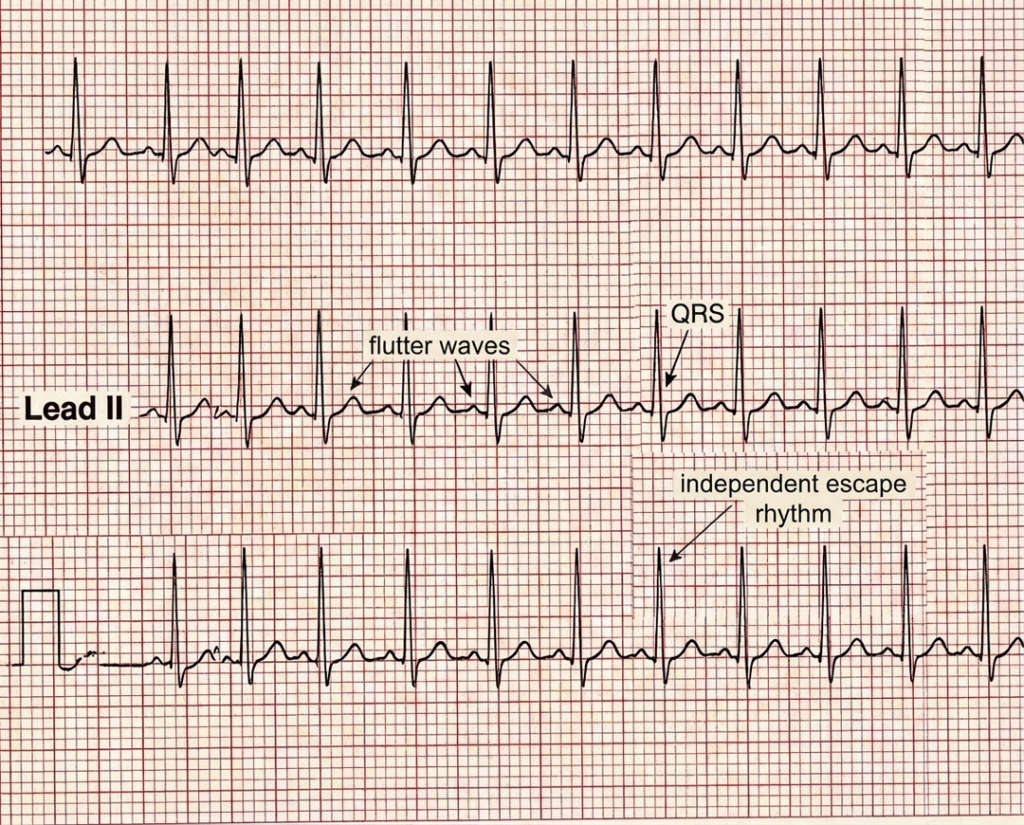
Variation 3: Atrial flutter activity with independent ventricular escape. Confirm AV dissociation by tracing atrial activity separately from QRS timing.
Tip: when the strip looks busy, first lock onto the atrial activity, then lock onto the ventricular activity, and finally confirm there is no consistent P to QRS relationship.
Diagnosis vs. Criteria: How do clinicians confirm complete heart block?
ECG criteria define the rhythm pattern, while diagnosis includes symptoms, stability, and evaluation for a reversible cause. Clinicians often confirm complete heart block by reviewing repeat ECGs and telemetry, checking vital signs and perfusion, reviewing medications that slow AV conduction, and assessing for ischemia or electrolyte abnormalities when indicated. Cardiology consultation is common because pacing may be required depending on stability and persistence.
Differential Diagnosis: AV Dissociation and Look Alikes
- Isorhythmic AV dissociation: atrial and ventricular rates may be similar but conduction is not truly linked.
- Junctional rhythm with retrograde P waves: P waves may occur after QRS but often in a consistent pattern.
- Ventricular tachycardia: may show AV dissociation but ventricular rate is typically fast with wide QRS.
- Atrial flutter with fixed block: flutter waves can be mistaken for P waves, look for sawtooth activity.
- Artifact: confirm true P waves across a longer strip or multiple leads.
Common Causes of Complete (3rd Degree) Heart Block
Complete heart block can result from reversible factors that temporarily impair conduction or irreversible damage to the conduction system.
Reversible Causes
- Medication effects: beta blockers, calcium channel blockers, digoxin
- Electrolyte imbalance, especially severe potassium or magnesium abnormalities
- Myocardial ischemia or myocardial infarction affecting the conduction system
- Inflammatory or infectious processes that may improve with treatment
Irreversible Causes
- Degenerative conduction disease and fibrosis within the conducting system
- Structural heart disease affecting the His-Purkinje system
- Post procedure or post-surgical injury to conduction pathways
- Infiltrative disease affecting cardiac conduction tissue
Clinical Signs and Symptoms
Symptoms depend on the ventricular escape rate and the patient’s ability to maintain perfusion. Slower escape rhythms produce lower cardiac output and more significant symptoms.
- Dizziness, fatigue, weakness
- Near syncope or syncope
- Shortness of breath or exercise intolerance
- Chest discomfort, especially if ischemia is present
- Hypotension, cool extremities, altered mental status
- Signs of heart failure in susceptible patients
Treatment Pathways for Third-Degree AV Block
Management depends on stability. The immediate goal is to support perfusion and treat symptomatic bradycardia while evaluating reversible causes. Persistent complete av block, as a critical atrioventricular av block subtype (often referred to as a third-degree av block), often requires pacing support.
- Initial stabilization: airway, oxygenation, monitoring, IV access
- Bradycardia pathway: follow ACLS and local protocol
- Atropine: may be less effective in infra nodal block but some protocols allow a trial
- Pacing: transcutaneous pacing for unstable patients, then transvenous pacing when needed
- Infusions: dopamine or epinephrine infusion as temporizing support per protocol
- Definitive therapy: evaluation for a permanent pacemaker if persistent or irreversible
- Correct causes: medication toxicity, ischemia, electrolyte abnormalities
Heart Block Poem
If the P’s and Q’s don’t agree,
Then you have that 3rd degree.
If the P waves march along,
And the QRS marches strong,
If the PR won’t stay the same,
And conduction plays no game,
If the atria beat on their own,
And ventricles have a rhythm grown,
If no impulse gets through cleanly,
That block is third degree completely.
3rd Degree Heart Block vs Mobitz II
| Rhythm Feature | 3rd Degree Heart Block | Mobitz II |
|---|---|---|
| P to QRS relationship | No consistent relationship, AV dissociation | Some P waves conduct with a consistent PR, then sudden dropped QRS |
| PR interval | Variable or not consistently measurable | Constant in conducted beats |
| Dropped beats | Not a dropped pattern, it is complete non conduction | Intermittent non conduction with dropped QRS complexes |
| Escape rhythm | Required to maintain ventricular activity | May be present if conduction ratio is low |
| Clinical risk | Often unstable, pacing frequently required | High risk of deterioration, pacing often indicated |
Frequently Asked Questions About 3rd Degree Heart Block
How serious is complete heart block?
It can be life threatening and lead to sudden cardiac arrest if the escape rhythm is too slow to maintain perfusion. Severity depends on symptoms, blood pressure, mental status, and escape rhythm stability.
How is pacemaker function monitored after implantation?
Pacemakers are monitored through scheduled device checks and remote monitoring when available. Clinicians assess sensing, pacing, lead function, battery status, and pacing percentages.
Can a heart block be prevented?
Some causes cannot be prevented, but risk can be reduced by managing cardiovascular risk factors, avoiding unnecessary AV nodal blocking medication combinations, and correcting reversible issues such as ischemia and electrolyte abnormalities.
If the block is below the AV node, is atropine still worth trying?
Atropine can be less effective in infra nodal blocks because it mainly improves av node conduction. Some protocols still allow a trial, but pacing is often the more reliable therapy when perfusion is compromised.
Summary
During a third-degree heart block, there’s no correlation between the P waves and QRS complexes. They both pulse at their own intrinsic rates. To treat the blockage, physicians must treat the underlying bradycardia.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
This article and video show An Easy Way to Interpret Arterial Blood Gases. Learn how to interpret arterial blood gases...
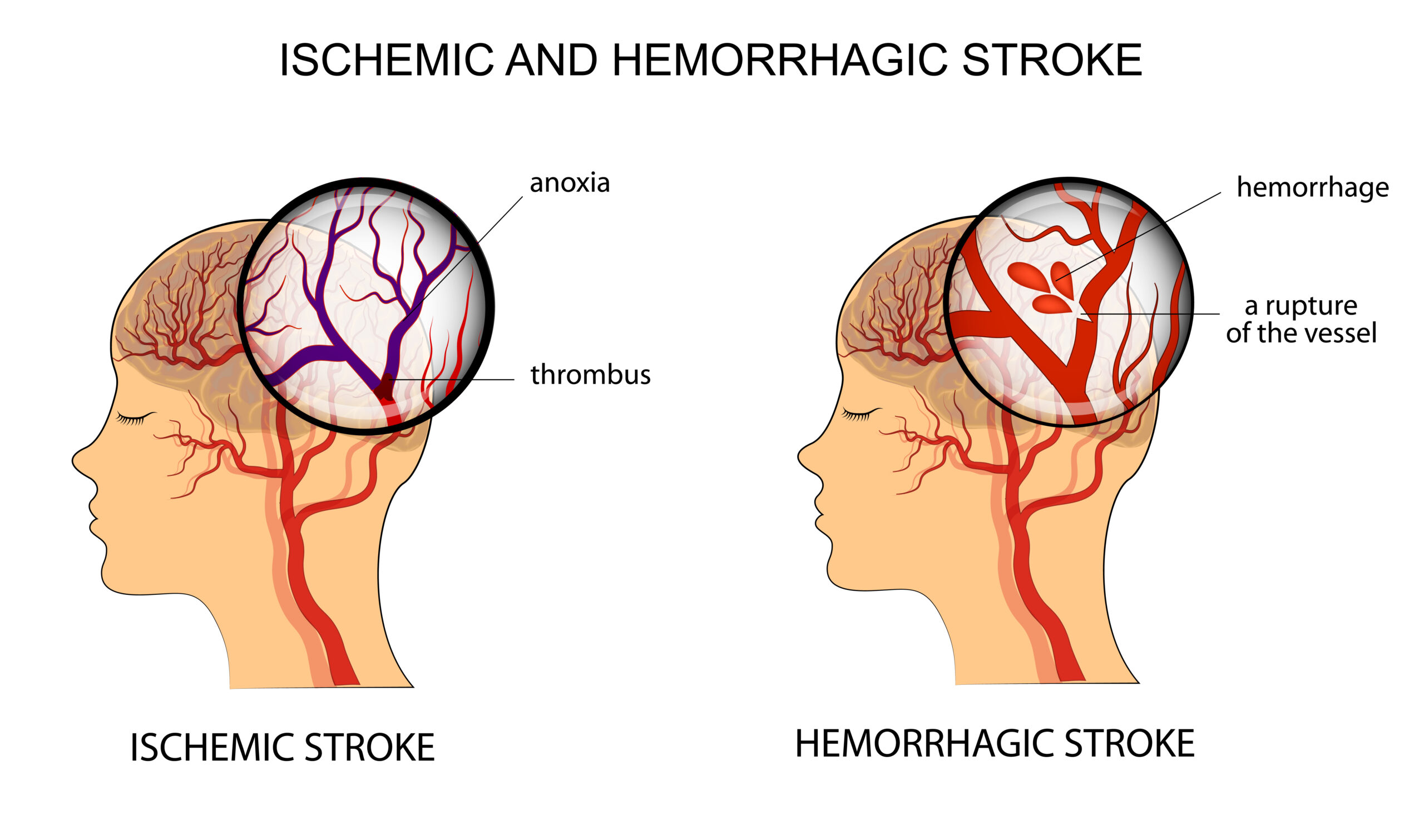
Learn the process of Acute Stroke Assessment in the Emergency Department. The general assessment is followed by Neurological assessment and determining ischemic or hemorrhagic stroke.