Adenosine in ACLS: Your Guide to Dosing, Indications, and Use for SVT
This guide explains how adenosine is used in ACLS for stable, regular narrow complex tachycardia, including when it is appropriate, how to give it correctly, and what to monitor for during administration. You will also learn dosing basics, pediatric considerations, adverse effects, and how adenosine compares with other SVT treatment options.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- Indicated for narrow-complex SVT, Adenosine is used to differentiate between SVT and VT or AF with RVR.
- Adenosine is contraindicated for wide, polymorphic VT.
- Adenosine affects the SA and AV nodes in the heart, causing temporary paralysis of these areas.
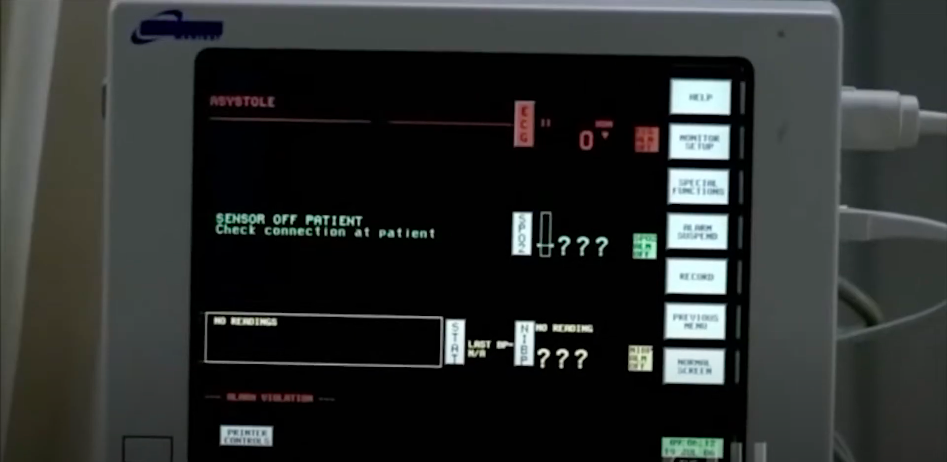
- The team should expect temporary asystole following administration.
- The first dose of adenosine is 6 mg IV and the second dose is 12 mg.
- The medication should be administered with a rapid IV push.
First, let’s review adenosine’s pharmacology and mechanism of action. Adenosine may sound familiar. If you’re thinking of adenosine from ATP (adenosine triphosphate), you’re exactly correct. Adenosine is found naturally within the body. When adenosine is synthesized, turned into a drug, and injected intravenously in large doses, several interesting events occur. Adenosine injection As it pertains to ACLS, adenosine affects the sinoatrial (SA) and the atrioventricular (AV) node, making it a cornerstone among ACLS drugs that you will learn about during your ACLS certification. Adenosine pumps potassium (K+) into the cells and inhibits calcium (Ca2+), in effect hyperpolarizing those areas of the heart. Adenosine temporarily paralyzes the SA node and the AV node. If one were to temporarily paralyze the whole top half of the heart, it would display on the cardiac monitor as a characteristic, yet temporary, asystole. Asystole on a cardiac monitor. In summary, adenosine impacts the SA node by inhibiting the SA node firing, which limits the conduction through the AV node.A Quick Overview of Adenosine
Mechanism of Action: How Adenosine Works
Indications of Adenosine
The following are ways adenosine is used in medical settings.
Therapeutic Use
Adenosine is the first drug of choice for a regular, narrow complex tachycardia, most notably supraventricular tachycardia (SVT). Before pushing the medication, clinicians must confirm the rhythm aligns with standard SVT ECG criteria, such as an absent P wave, narrow QRS complex, and highly regular rate. Adenosine “stops” the heart just long enough to terminate SVTs.
SVT Criteria: What to Look for on the ECG
This video supports the therapeutic use section by reviewing ECG findings that help identify SVT and confirm when adenosine is an appropriate first line option in a stable, regular narrow complex rhythm.
These tachycardias are usually caused by a re-entry problem. The conduction travels through the atrium, arrives around the AV node, and then part of the conduction loops back into the atrium. It re-enters the heart. It “cuts in line” and begins another impulse.
The re-entry point for most narrow complex SVTs is at the AV node. Fortunately, adenosine works right at the AV node. That’s why it’s so effective in treating supraventricular tachycardias.
Adenosine Administration for SVT: Practical Treatment Walkthrough
This video demonstrates how adenosine is given during SVT treatment, including timing, monitoring, and what rhythm changes to expect immediately after a rapid IV push.
Suppose your patient has a heart rate clipping along at 182–220 bpm. Maybe you’re having a hard time discerning whether this is regular or irregular. Is this a regular supraventricular tachycardia or an atrial fibrillation with a rapid ventricular response? It’s hard to distinguish because the R waves occur so rapidly.
AF with RVR vs SVT: Avoiding the Common Misread
This video helps you differentiate SVT from atrial fibrillation with rapid ventricular response. That matters because adenosine may briefly slow AV nodal conduction to clarify the rhythm but it will not terminate atrial fibrillation.
Now, suppose you administer adenosine, and it doesn’t work. Adenosine is ineffective in treating atrial fibrillation. In atrial fibrillation, other re-entry pathways are being used besides the AV node. If adenosine works on the AV node, it’s not going to impact the other re-entry ports used during atrial fibrillation with a rapid ventricular response (RVR).
Read: 10 Cardiac Drugs to Know for the Pharmacology Test
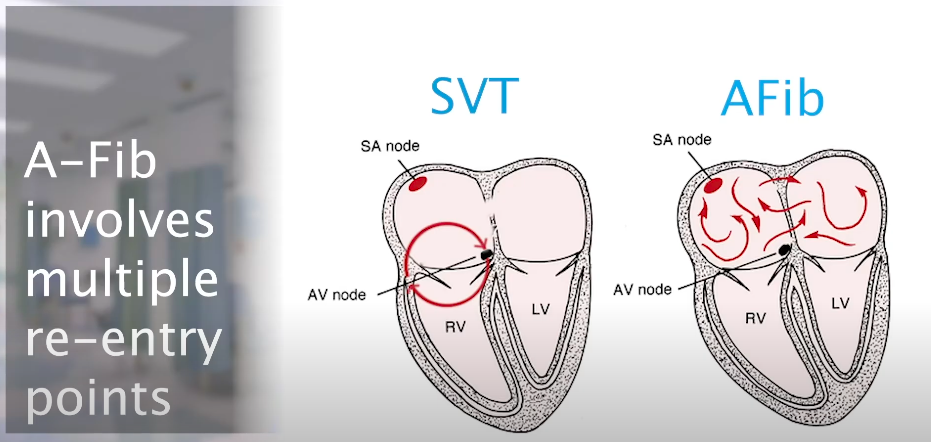
The SVT reentry pathway is typically the AV node, while re-entry pathways vary in atrial fibrillation.
Diagnostic Use
Adenosine is a first-line drug for narrow complex, regular supraventricular tachycardias (SVT). Adenosine is also used as a diagnostic drug for ventricular tachycardia (VT).
Remember, adenosine won’t treat the cause of VT. It impacts the SA node while VT originates in the ventricular chambers, so adenosine won’t work. However, you can use adenosine as a diagnostic tool to discern between VT or SVT with an aberrant ventricular conduction.
Additionally, if your patient is stable, obtain a 12-lead EKG rather than administering adenosine. The EKG provides the same information.
Dosing
The first dose of adenosine for SVT is a 6mg rapid IV push. If the heart rate does not convert within a minute or so, administer an additional 12 mg. So, you’ll initially administer 6 mg followed by a 12 mg IV push.

Supraventricular Tachycardia Adenosine Dosing
Pediatric dosing guidance
In pediatric patients with stable, regular narrow complex SVT, adenosine dosing is weight based and should be administered as a rapid IV or IO push followed immediately by a normal saline flush. Use the most proximal access available when possible to ensure the medication reaches the heart quickly.
- First dose: 0.1 mg per kg (maximum 6 mg)
- Second dose: 0.2 mg per kg (maximum 12 mg)
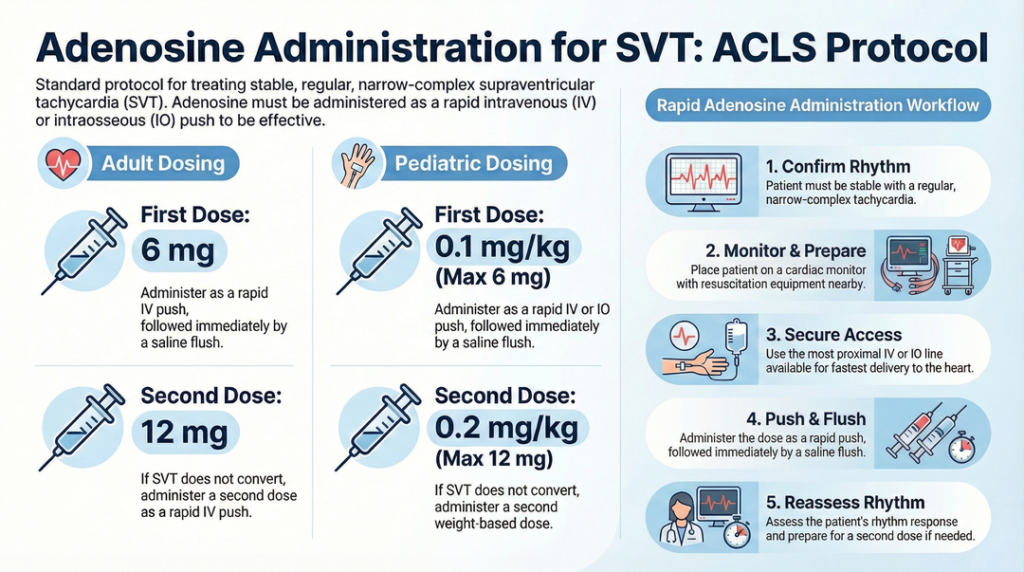
Adenosine dosing in ACLS for supraventricular tachycardia, including adult and pediatric weight-based dosing and rapid administration workflow.
Rapid administration steps (quick flow)
Adenosine administration workflow
- Confirm the rhythm is regular and narrow complex, and the patient is stable.
- Place the patient on a monitor and have resuscitation equipment ready.
- Use the most proximal IV or IO access available.
- Prepare an adenosine dose and a normal saline flush.
- Push adenosine rapidly, then flush immediately.
- Assess rhythm response and repeat dosing if indicated.
Adverse Effects and Contraindications
Expected transient effects
Adenosine commonly causes brief flushing, chest pressure, shortness of breath, lightheadedness, or a sense of impending doom. These effects are usually short lived because the medication is cleared rapidly.
When to avoid or use extra caution
- Irregular or polymorphic wide complex tachycardia: avoid adenosine when the rhythm suggests polymorphic VT.
- Reactive airway disease: use caution due to risk of bronchospasm.
- Heart transplant patients: they may be more sensitive to adenosine and may require lower dosing per local protocol.
- Drug interactions: methylxanthines like caffeine and theophylline may reduce effect, while dipyridamole can increase effect.
Polymorphic VT (Torsades de Pointes) recognition
This video reviews torsades de pointes and other polymorphic ventricular tachycardia patterns where adenosine is not an appropriate treatment choice.
Metabolism and Clinical Implications
Adenosine has an extremely short half life, which is why it must be given as a rapid IV or IO push followed immediately by a flush. It is rapidly taken up and metabolized in the blood and vascular tissues, so slow administration can make the dose ineffective before it reaches the AV node.
- Use a proximal line when possible.
- Use a rapid push technique and flush immediately.
- Expect a brief rhythm pause or transient AV block on the monitor.
Adenosine vs Other Antiarrhythmics for SVT
Adenosine is typically used for stable, regular narrow complex SVT because it acts quickly and can both treat and clarify rhythms. Other options may be used depending on the rhythm type, patient stability, and contraindications.
| Option | Best use case | Onset and duration | Key cautions |
|---|---|---|---|
| Adenosine | Stable, regular narrow complex SVT | Very fast onset, very short duration | Not for polymorphic wide complex rhythms, caution in bronchospasm risk |
| Vagal maneuvers | First step in stable SVT | Immediate if effective | May be less effective in some patients |
| AV nodal blockers | Selected stable SVT situations per protocol | Slower onset, longer duration | Avoid in unstable patients, watch for hypotension |
| Synchronized cardioversion | Unstable tachycardia or refractory cases | Immediate | Requires sedation when possible and correct synchronization |
Adenosine inhibits the SA node firing and conduction through the AV node. It’s used to treat SVTs. It may also be used as a diagnostic tool in the case of ventricular tachycardias. Remember to administer a liberal amount due to its short half-life.Summary
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn
This article and video detail Shock: Cardiogenic, Hypovolemic, and Septic. Learn the three common types of shock, pathophysiology...
This article and video show An Easy Way to Interpret Arterial Blood Gases. Learn how to interpret arterial blood gases...