First-Degree Heart Block
First degree heart block is a conduction delay between the atria and ventricles, most commonly at the AV node. On ECG, it is defined by a prolonged PR interval that stays consistent from beat to beat. This page explains exactly how to measure the PR interval, how to recognize mild versus marked PR prolongation, and what the finding may mean clinically.
ACLS Certification Association videos have been peer-reviewed for medical accuracy by the ACA medical review board.
Article at a Glance
- First-degree heart block is characterized by:
- Regularity: Depends on underlying rhythm
- Rate: Depends on underlying rhythm
- P Wave: Uniform with one for every QRS
- PR Interval: > 0.20 seconds and consistent
- QRS Complex: < 0.12 seconds
Criteria for Determining a First Degree Heart Block
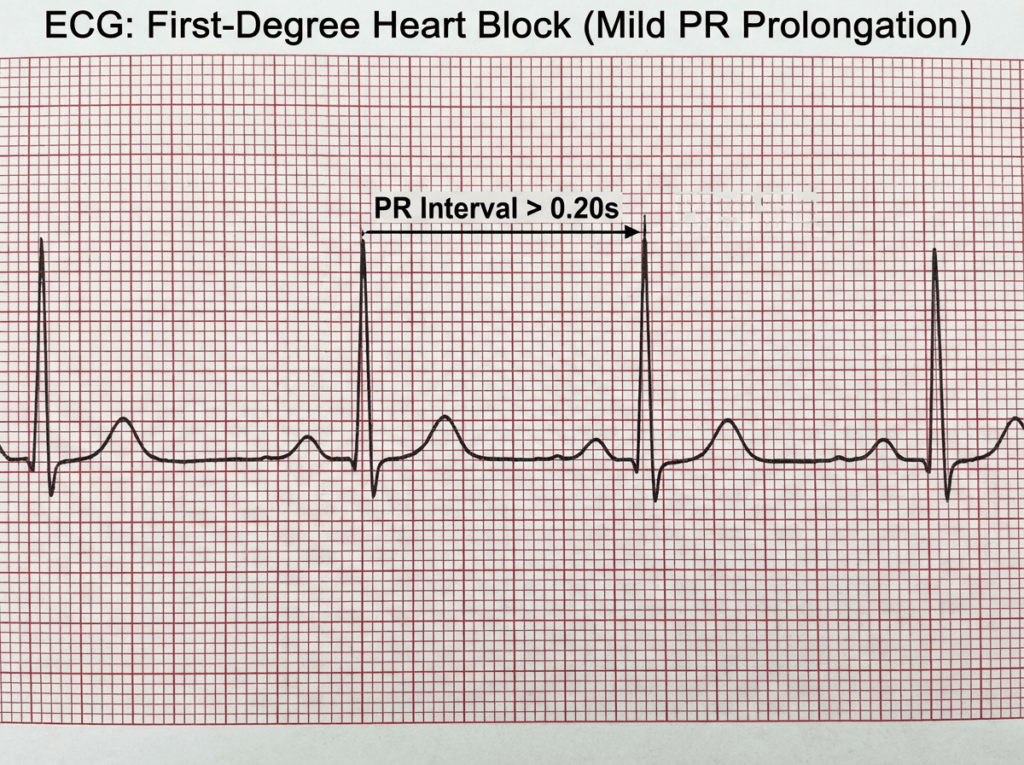
We must examine the relationship between the P wave and QRS complex. A normal PR interval (PRI) is between 0.12 and 0.20 seconds. A first-degree heart block occurs when the PR interval is greater than 0.20 seconds.
The second largest box on an ECG paper measures 0.20 seconds. Locate a P wave that starts right on that box, and if the QRS occurs after the beginning of the next box, there’s a first-degree heart block.
To identify first degree heart block, focus on the PR interval, which represents the time from atrial depolarization to the beginning of ventricular depolarization. The PR interval is measured from the start of the P wave to the start of the QRS complex.
Normal PR interval: 0.12 to 0.20 seconds (120 to 200 ms).
First degree heart block: PR interval greater than 0.20 seconds, with every P wave followed by a QRS complex and a constant PR interval from beat to beat.
How to measure the PR interval on ECG paper
- Choose a clear lead where the P wave and QRS are easy to see (often lead II).
- Mark the start of the P wave and the start of the QRS complex.
- Count small boxes between those two points.
- At 25 mm/s, each small box equals 0.04 seconds.
- Each large box equals 0.20 seconds.
- If the PR interval is longer than one large box (more than 0.20 seconds), the ECG meets criteria for first degree heart block.
Marked first degree heart block
Some ECGs show a very prolonged PR interval, sometimes called marked first degree heart block (often PR 0.30 seconds or longer). This can be more clinically significant, especially if the patient is symptomatic or taking AV nodal blocking medications.
How it differs from other AV blocks
- First degree: PR interval is prolonged but every P wave conducts to a QRS.
- Second degree: some P waves do not conduct, so QRS complexes are intermittently dropped.
- Third degree: complete AV dissociation, with atrial activity and ventricular activity occurring independently. This can be clearly seen on an ECG, often referred to as a third degree heart block strip.
ECG Strip: First Degree Heart Block
This video walks through a first degree heart block ECG strip and shows how to identify a prolonged PR interval while confirming that every P wave still conducts to a QRS complex. Use it as a visual reference while you practice measuring PR intervals on your own strips.
First degree heart block example with a consistently prolonged PR interval.

Marked first degree heart block example with a markedly prolonged PR interval.
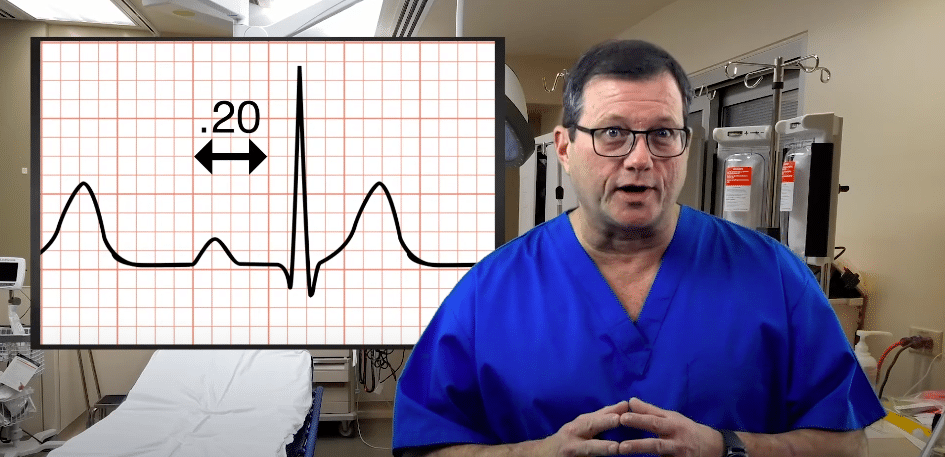
The QRS complex occurs after the beginning of the second box, so we know the PRI is greater than 0.20 seconds.
A first-degree heart block is usually benign and asymptomatic. You should still keep an eye on it, as it points to a conduction problem somewhere, potentially around the AV node.
What Causes First Degree Heart Block?
First degree heart block occurs when conduction between the atria and ventricles slows, most often at the AV node. In many people it is an incidental ECG finding, but it can also be associated with medications or underlying heart disease.
Common causes and contributing factors
- Increased vagal tone (often in athletes or during rest and sleep)
- Medications that slow AV nodal conduction, such as beta blockers, non dihydropyridine calcium channel blockers, digoxin, and some antiarrhythmics
- Ischemia or infarction, especially involving the inferior wall where AV nodal blood supply may be affected
- Structural or degenerative conduction disease that increases with age
- Myocarditis or inflammatory conditions affecting conduction tissue
- Electrolyte abnormalities and metabolic issues that can slow conduction
If first degree heart block is new or accompanied by symptoms, review medication changes, assess for ischemia when clinically indicated, and consider broader causes based on the clinical context.
Symptoms of First Degree Heart Block
Most patients with first degree heart block have no symptoms. The rhythm is often discovered incidentally on a screening ECG or during evaluation for an unrelated concern.
When symptoms may occur
Symptoms are more likely if the PR interval is markedly prolonged or if there is an additional conduction abnormality. Some patients may report:
- Fatigue or reduced exercise tolerance
- Lightheadedness, especially with exertion
- Palpitations or an awareness of slow or irregular beats
Symptoms should always be interpreted in context. If a patient is symptomatic, evaluate for other causes and consider whether medications or progression to a higher degree AV block may be contributing.
How is First Degree Heart Block Diagnosed?
The primary diagnostic tool for first degree heart block is the 12 lead ECG. Diagnosis is confirmed when the PR interval is greater than 0.20 seconds and every P wave is followed by a QRS complex.
What clinicians look for on ECG
- Consistent PR prolongation across beats
- One to one AV conduction without dropped QRS complexes
- Any additional findings, such as bundle branch block or ischemic changes, that may suggest broader conduction system disease
Supportive tests when clinically appropriate
Depending on the patient and symptoms, clinicians may also consider:
- Medication review and basic labs for electrolytes and thyroid function
- Cardiac biomarkers and further evaluation if ischemia is suspected
- Ambulatory monitoring if symptoms are intermittent
- Echocardiography if structural heart disease is suspected
Treatment and Management of First Degree Heart Block
In most cases, first degree heart block does not require specific treatment. Management typically focuses on monitoring, addressing reversible contributors, and evaluating symptoms when they are present.
Typical management approach
- Asymptomatic patients: reassurance and routine follow up as clinically indicated
- Medication related PR prolongation: review AV nodal blocking drugs and adjust if needed based on symptoms and provider judgement
- New onset PR prolongation: evaluate for ischemia, myocarditis, electrolyte issues, or conduction disease when appropriate
When closer evaluation may be needed
Consider further evaluation if the patient has symptoms, marked PR prolongation, coexisting bundle branch block, or evidence of progression toward higher degree AV block.
Prognosis and Potential Complications
First degree heart block is often benign, especially when it is isolated and the patient is asymptomatic. However, it can signal slowed conduction in the AV node or broader conduction system disease, so clinical context matters.
Potential considerations over time
- Progression to higher degree AV block in some patients, particularly with underlying conduction disease
- Association with other cardiac conditions depending on the cause, such as ischemic heart disease
- Greater clinical relevance when PR prolongation is marked or when symptoms develop
If the PR interval becomes progressively longer, symptoms develop, or additional conduction abnormalities appear, further clinical evaluation is warranted.
Summary
First degree heart block is identified on ECG when the PR interval is greater than 0.20 seconds while every P wave still conducts to a QRS complex. Accurate diagnosis depends on correct PR measurement and differentiation from higher degree AV blocks that drop beats or show AV dissociation.
Most cases are asymptomatic and do not require treatment. Management focuses on clinical context, reviewing AV nodal blocking medications, and monitoring when the finding is new, marked, or associated with symptoms. Understanding potential causes and prognosis helps clinicians recognize when simple observation is appropriate and when additional evaluation may be needed.
More Free Resources to Keep You at Your Best
Editorial Note
ACLS Certification Association (ACA) uses only high-quality medical resources and peer-reviewed studies to support the facts within our articles. Explore our editorial process to learn how our content reflects clinical accuracy and the latest best practices in medicine. As an ACA Authorized Training Center, all content is reviewed for medical accuracy by the ACA Medical Review Board.
More to Learn

Download the Tachycardia with a Pulse Algorithm PDF. The assessment and treatment of patients with a heart rate higher than 150 beats per minute is also presented in a video.
This article and video explain the Dosage Calculations. Learn the 5 steps to calculate your dosages.