Cardiac Blocks Flashcard
Rationale
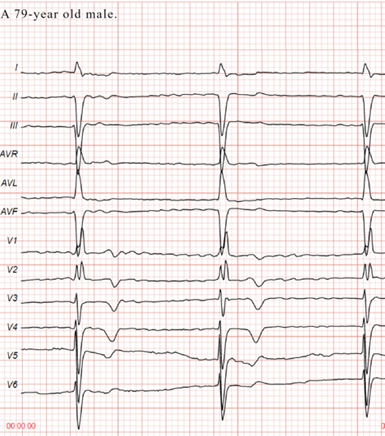
D. Rationale: There is an rsR’ pattern in leads V1 and V2 with broad terminal or “slurred” S waves in the lateral precordial leads V4 to V6, which is indicative of complete right bundle branch block.
Answer choice A – In complete heart block, there is an absence of atrioventricular conduction whereby patients will present with severe bradycardia and independent atrial and ventricular rates.
Answer choice B – When there is an incomplete left bundle branch block, the patient will present with ECG changes consistent with the typical left bundle branch block morphology such as a dominant S wave in V1, a broad monophasic R wave in the lateral leads, and the absence of Q waves in the lateral leads, but with a QRS duration < 120 ms.
Answer choice C – In sick sinus syndrome, the abnormal sinus node function will result in symptomatic bradycardia, sinus arrest, or exit block.
Question
A 79-year-old man presents with severe bradycardia and the ECG tracing seen below. Aside from the bradycardia, what is the most striking ECG diagnosis one can conclude in this patient?
a. Complete atrioventricular block
b. Incomplete left bundle branch block
c. Sick sinus syndrome
d. Complete right bundle branch block
Answer
d. Complete right bundle branch block
Rationale
C. Rationale: Left anterior fascicular blocks potentially mask inferior wall and anterior wall STEMI.
Question
Due to its delay in conduction, a left anterior fascicular block potentially masks which one of the following?
a. Anteroseptal wall myocardial infarction
b. Septal wall myocardial infarction
c. Inferior wall myocardial infarction
d. Lateral wall myocardial infarction
Answer
c. Inferior wall myocardial infarction
Rationale
B. Rationale: A left BBB produces tall R waves in the lateral leads; leads I and V5–V6.
Answer choice A – Left BBB produces deep S waves in the precordial leads, V1–V3.
Answer choice C – Tall, peaked T waves typically represent hyperkalemia.
Answer choice D – Inverted T waves represent myocardial ischemia.
“
Question
How will a left bundle branch block manifest on ECG?
a. Small s waves in leads II, III, and aVF
b. Tall R waves in the lateral leads
c. Tall, peaked T waves in all leads
d. Inverted T waves in limb leads
Answer
b. Tall R waves in the lateral leads
Rationale
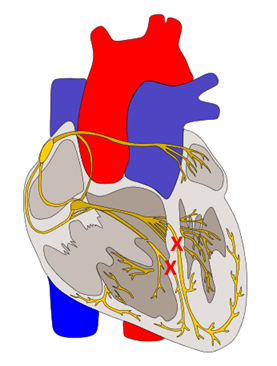
D. Rationale: The image represents a bifascicular block of the right bundle branch with a left anterior fascicular block variant. The ‘X’ represents the block at the right bundle branch and at the left anterior fascicle. ECG findings in this bilateral fascicular block include a QRS duration > 120 ms; rsR’ complex in V1, which is typically seen in right bundle-branch block; left axis deviation; small q waves in lead aVL; rS complex in leads II, III, and aVF with positive T waves; and a clockwise rotation in the precordial leads.
Answer choice A – Right axis deviation would manifest as a dominant R wave in leads II, III, and AVF.
Answer choice B – A short PR interval would manifest as a PR interval < 0.12 seconds.
Answer choice C – A bilateral fascicular block would manifest as a counterclockwise rotation in the precordial leads.
Question
The red “X” marks on the image below depict the site of a bilateral fascicular block. Which one of the following choices is an ECG finding characteristic of this type of bilateral fascicular block?
a. Right axis deviation
b. Short PR interval
c. Counterclockwise rotation in precordial leads
d. Left axis deviation
Answer
d. Left axis deviation
Rationale
A. Rationale: Incomplete right bundle-branch block is commonly seen in young patients. There is a notching in the QRS complex described as an rSr’ pattern.
Answer choices B & C – ST elevation and ST depression indicate coronary artery disease.
Answer choice D – The presence of a delta wave represents pre-excitation syndromes such as Wolff-Parkinson-White syndrome.
Question
Which of the following ECG characteristics represents an incomplete right bundle-branch block?
a. An rSr’ in frontal lead III
b. ST elevation in precordial lead V3
c. ST depression in frontal lead aVF
d. The presence of a delta wave
Answer
a. An rSr’ in frontal lead III
Rationale
D. Rationale: The diagnostic criteria of right bundle branch block include a broad QRS complex, an rsR’ in precordial leads V1–V3, and wide slurred S waves in lateral leads I, aVL, and V5–V6. These findings are brought about by the higher magnitude of impulses from the left ventricular depolarizations than the right ventricular depolarizations.
Question
Which one of the following diagnostic criteria indicates right bundle branch block?
a. Broad QRS complex
b. rsR’ pattern in precordial leads V1–V3
c. Wide slurred S waves in leads I, aVL, V5–V6
d. All of the above
Answer
d. All of the above
Rationale
D. Rationale: Studies have shown that an isolated left posterior fascicular block is most likely produced by an inferior wall myocardial infarction.
Answer choice A – An isolated left anterior fascicular block is most likely caused by left ventricular hypertrophy.
Answer choice B – Fibrosis of the infrahisian conduction system known as Lenégre disease most likely causes an isolated left anterior fascicular block.
Answer choice C – A pulmonary embolism most likely causes right ventricular hypertrophy with an isolated right fascicular block.
Question
Which one of the following disease processes is more likely to produce a left posterior fascicular block than a left anterior fascicular block?
a. Left ventricular hypertrophy
b. Lenégre disease
c. Pulmonary embolism
d. Inferior wall myocardial infarction
Answer
d. Inferior wall myocardial infarction
Rationale
A. Rationale: Inferior wall MI is associated with left posterior fascicular block, particularly if the frontal QRS axis is between +50° and +140°. Left posterior fascicular block masks the classic ECG characteristics of myocardial infarction.
Answer choice B – Ventricular tachycardia is a dysrhythmia that is unassociated with left posterior fascicular block.
Answer choice C – Wolff-Parkinson-White syndrome is a disorder in which an extra electrical pathway produces a very rapid heartbeat.
Answer choice D – Torsade’s de pointes is a dysrhythmia associated with low magnesium levels.
Question
Which one of the following diseases of the heart is commonly associated with a left posterior fascicular block?
a. Inferior wall MI
b. Ventricular tachycardia
c. Wolff-Parkinson-White syndrome
d. Torsade’s de pointes
Answer
a. Inferior wall MI
Rationale
D. Rationale: The trifascicular block involves the right bundle branch, left anterior fascicle, and left posterior fascicle. The conduction of impulses is maintained if there is the presence of an atypical medial fascicle located in between the left anterior and left posterior fascicles. However, patients may develop a complete atrioventricular block at any time.
Question
Which one of the following infrahisian conduction systems is NOT involved in a trifascicular block?
a. Right bundle branch
b. Left anterior fascicle
c. Left posterior fascicle
d. Medial fascicle
Answer
d. Medial fascicle